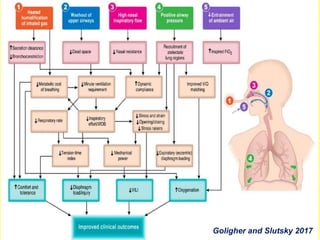
HFNC therapy provides high flow oxygen through a nasal cannula. It has several benefits over traditional oxygen delivery methods, including more accurate oxygen delivery, washout of dead space, and generation of positive end-expiratory pressure. HFNC is a well-tolerated therapy that can be used for hypoxemic respiratory failure, pre-intubation, and post-extubation. While promising, further research is still needed to establish clear guidelines for its use.






























![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)











![oxygen therapy in covid-19 patients the role of hfnc and cpap (ferrari) [r]](https://cdn.slidesharecdn.com/ss_thumbnails/icummp2021-oxygentherapyincovid-19patientstheroleofhfncandcpapferrarir-210909214721-thumbnail.jpg?width=640&height=640&fit=bounds)




















































