Downloaded 600 times
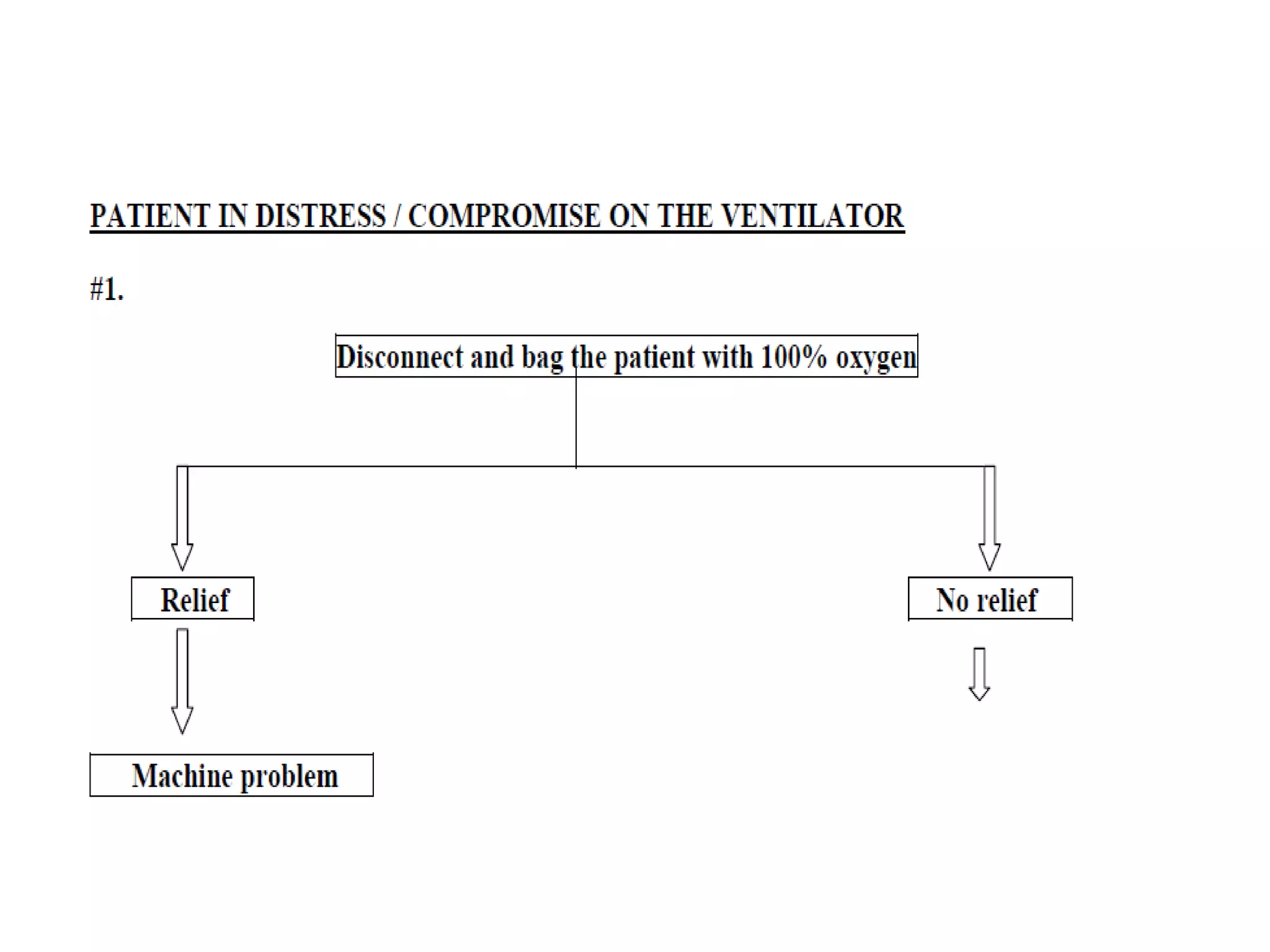
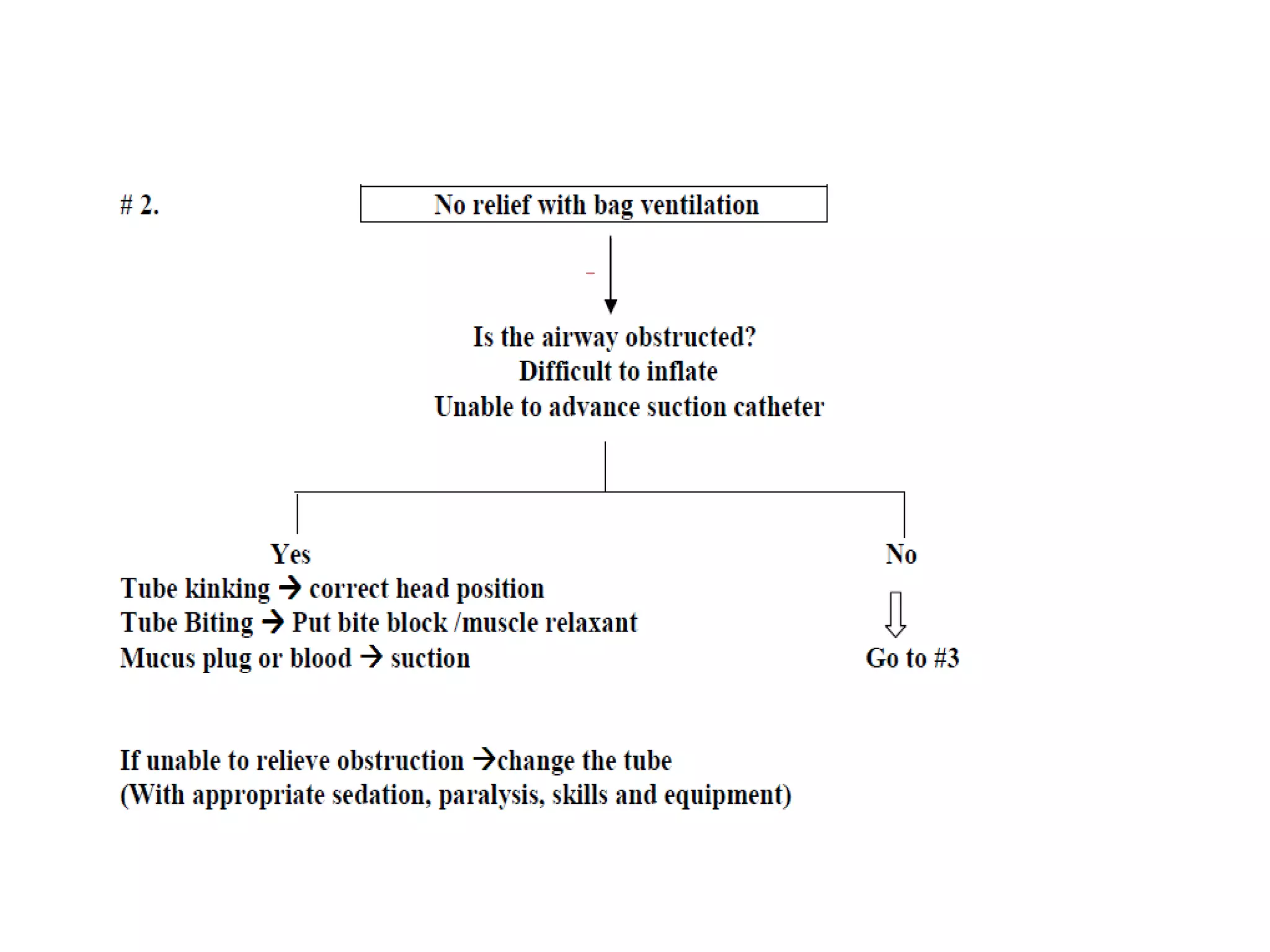
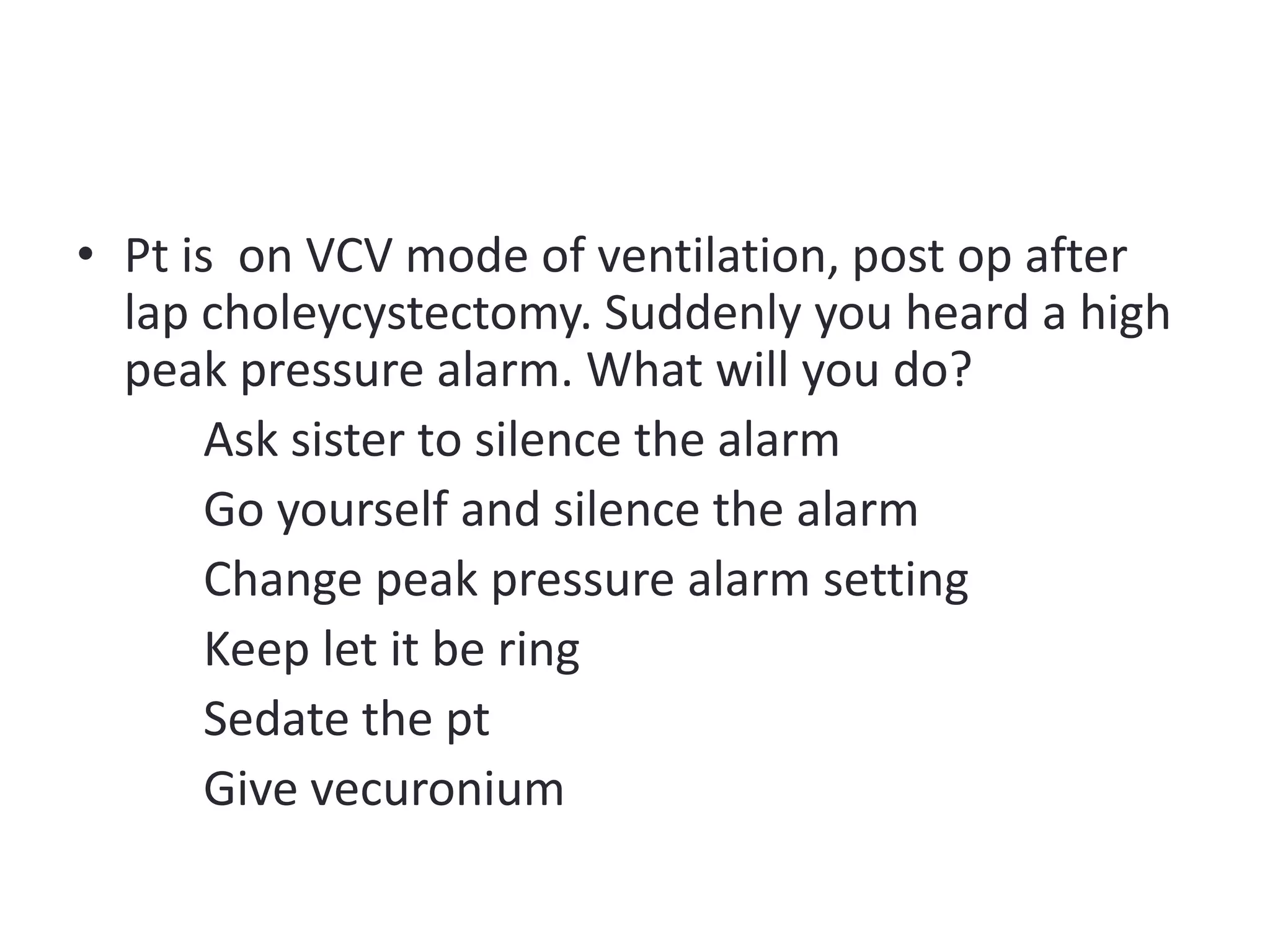



The document provides guidelines for troubleshooting mechanical ventilators, emphasizing key precautions regarding power supply, gas sources, and personnel training. It details the importance of regular servicing, alarm recognition, and proper response to various alarm conditions. Additionally, it includes specific troubleshooting steps for high and low pressure alarms and practical case scenarios for critical interventions.













































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)









