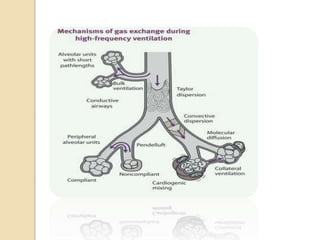
High frequency oscillatory ventilation (HFOV) delivers very small, high frequency breaths to open collapsed alveoli and improve gas exchange. It maintains a constant high mean airway pressure to prevent alveolar collapse and uses smaller tidal volumes to reduce lung injury compared to conventional ventilation. Gas exchange occurs through several mechanisms, including bulk flow, gas mixing through oscillations, and diffusion. Practitioners adjust the mean airway pressure, amplitude, and frequency to control oxygen and carbon dioxide levels. HFOV is used as a rescue therapy for severe ARDS and lung injury when conventional ventilation fails. Potential complications include pneumothorax, hemodynamic effects, infection risks, and difficulties with transport and monitoring.