Downloaded 88 times

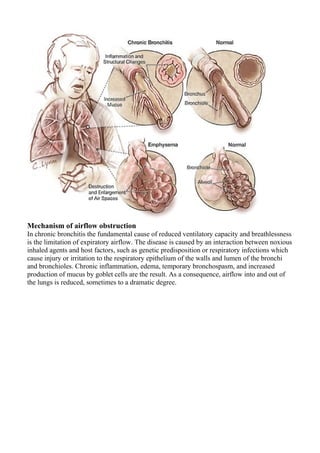


Chronic Bronchitis is a respiratory condition characterized by persistent cough and sputum production for at least three months per year caused by inflammation of the bronchial tubes. It is usually caused by long-term cigarette smoking which damages the airways and increases mucus production over many years. The primary symptoms include a daily cough with sputum, worsening shortness of breath, and reduced ability to exercise. While restoration of normal lung function is not possible, treatment aims to reduce symptoms and disability by addressing airway obstruction, infections, oxygen levels, and encouraging smoking cessation.











































































































