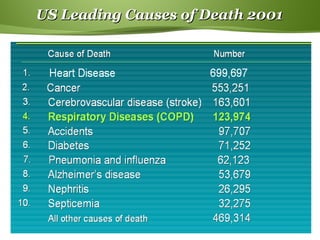
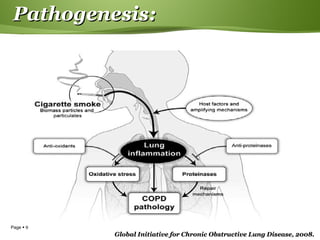
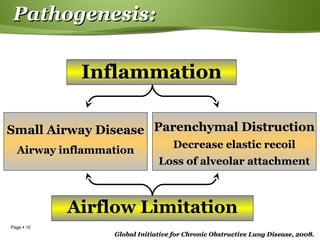
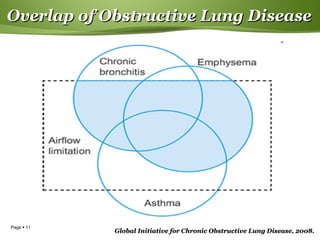
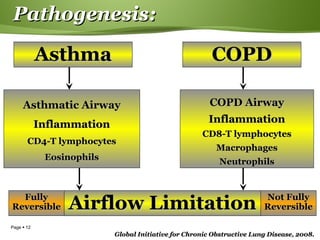
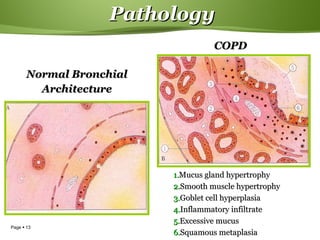
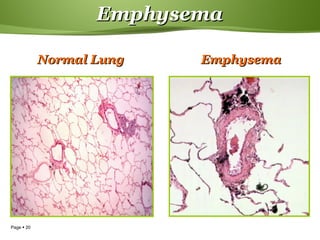
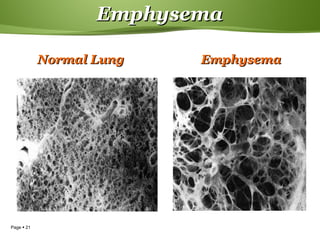
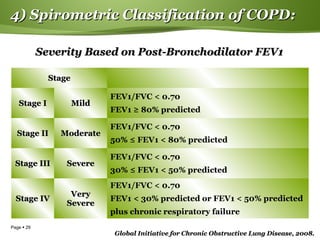
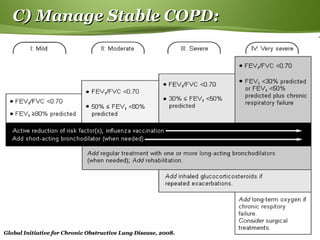
This document provides information on chronic obstructive pulmonary disease (COPD). It discusses the epidemiology, definition, risk factors, pathogenesis, pathology, classification, management, and exacerbations of COPD. Key points include: cigarette smoking is the primary cause of COPD worldwide; the disease involves inflammation in the lungs from noxious particles leading to airflow limitation; emphysema and chronic bronchitis are the major pathological changes; severity is classified based on lung function tests; and management involves reducing risk factors, treating stable COPD, and managing exacerbations.