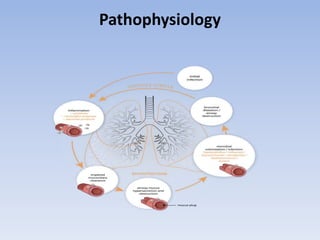
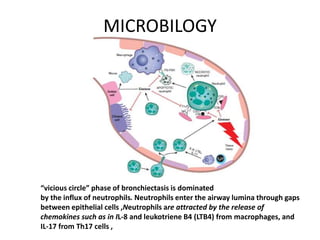
Bronchiectasis has a variety of etiologies including prior lung infections, genetic disorders affecting cilia or cartilage, and inflammatory conditions. The pathophysiology involves a vicious cycle of infection and inflammation that destroys the bronchial walls. Chronic neutrophilic inflammation from bacterial toxins causes tissue damage through proteolytic enzymes. This further impairs mucociliary clearance and predisposes the individual to recurrent infections that perpetuate the cycle of inflammation and lung damage leading to bronchiectasis.








































































































![ergonomics[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ergonomics1-230226092320-24f170c5-thumbnail.jpg?width=640&height=640&fit=bounds)






















