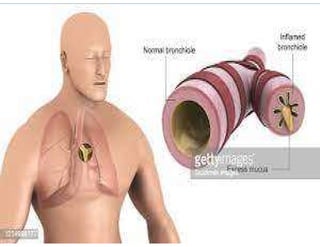
The document provides a comprehensive overview of bronchitis, including its definition, types (acute and chronic), and management strategies. It describes the causes, pathophysiology, symptoms, diagnosis, treatment, and potential complications associated with bronchitis. Additionally, it outlines nursing care, preventive measures, and educational guidance for patients suffering from this respiratory condition.