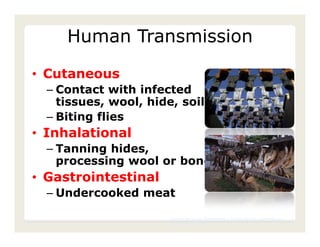
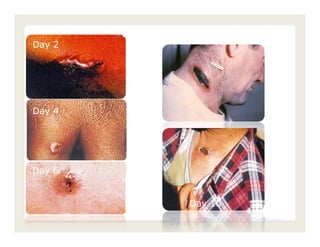
Bacillus anthracis is the bacterium that causes anthrax. It forms spores that are highly resistant to heat, cold, and chemicals. Anthrax spores can survive for decades in the soil and infect mammals. The disease can be transmitted to humans through contact with infected animals, animal products, or inhalation of anthrax spores. Anthrax infections cause skin lesions, severe gastrointestinal illness, or deadly hemorrhagic pneumonia depending on the route of exposure. Prompt antibiotic treatment can cure anthrax if caught early.














































![[Micro] gram positive spore bearing rods](https://cdn.slidesharecdn.com/ss_thumbnails/xi8ojr00samkfuo2qtsz-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)













































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













