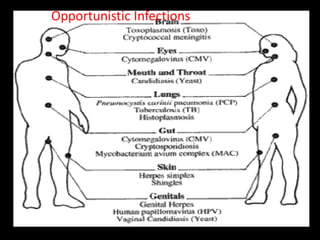
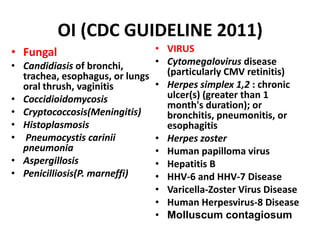
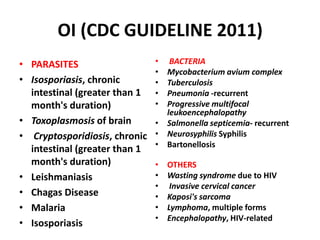
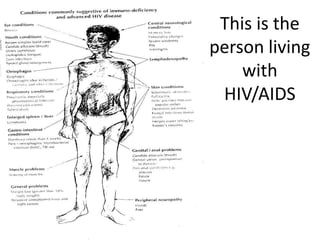
Opportunistic infections are infections that occur more frequently and are more severe in people with weakened immune systems such as those with HIV/AIDS. These infections include fungal, bacterial, viral, and parasitic infections that typically do not seriously affect those with healthy immune systems. Common opportunistic infections in HIV/AIDS patients include Pneumocystis pneumonia, tuberculosis, candidiasis, toxoplasmosis, cryptococcus, and cytomegalovirus. Antiretroviral therapy has significantly reduced the rates of opportunistic infections by suppressing HIV and allowing immune recovery. HIV/AIDS remains a major global public health challenge.