Downloaded 245 times


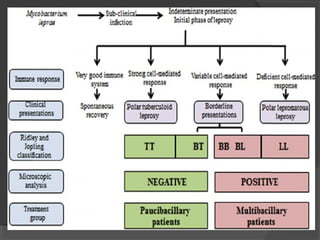



This document provides information about leprosy (Hansen's disease), including: - It is caused by Mycobacterium leprae and primarily affects the skin, nerves, and mucosa. - There are several classification systems including paucibacillary, multibacillary, lepromatous, tuberculoid, and borderline. Classification depends on immune response and bacterial load. - It remains a major public health problem with millions of cases worldwide, especially in India, Brazil, and African countries. Treatment involves multidrug therapy to prevent disability.









































































