Downloaded 350 times


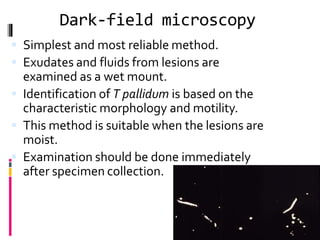


Treponema pallidum is a spirochete bacterium that causes syphilis. It is thin and delicate, about 10 micrometers in length, and actively motile. T. pallidum cannot be grown in culture but can be seen microscopically using dark-field illumination or silver staining. Syphilis has stages including primary, secondary, latent, and tertiary, and can involve multiple organs if untreated. Diagnosis involves microscopic examination of samples or serological tests to detect antibodies. Penicillin is the treatment of choice.























































































