Downloaded 1,252 times







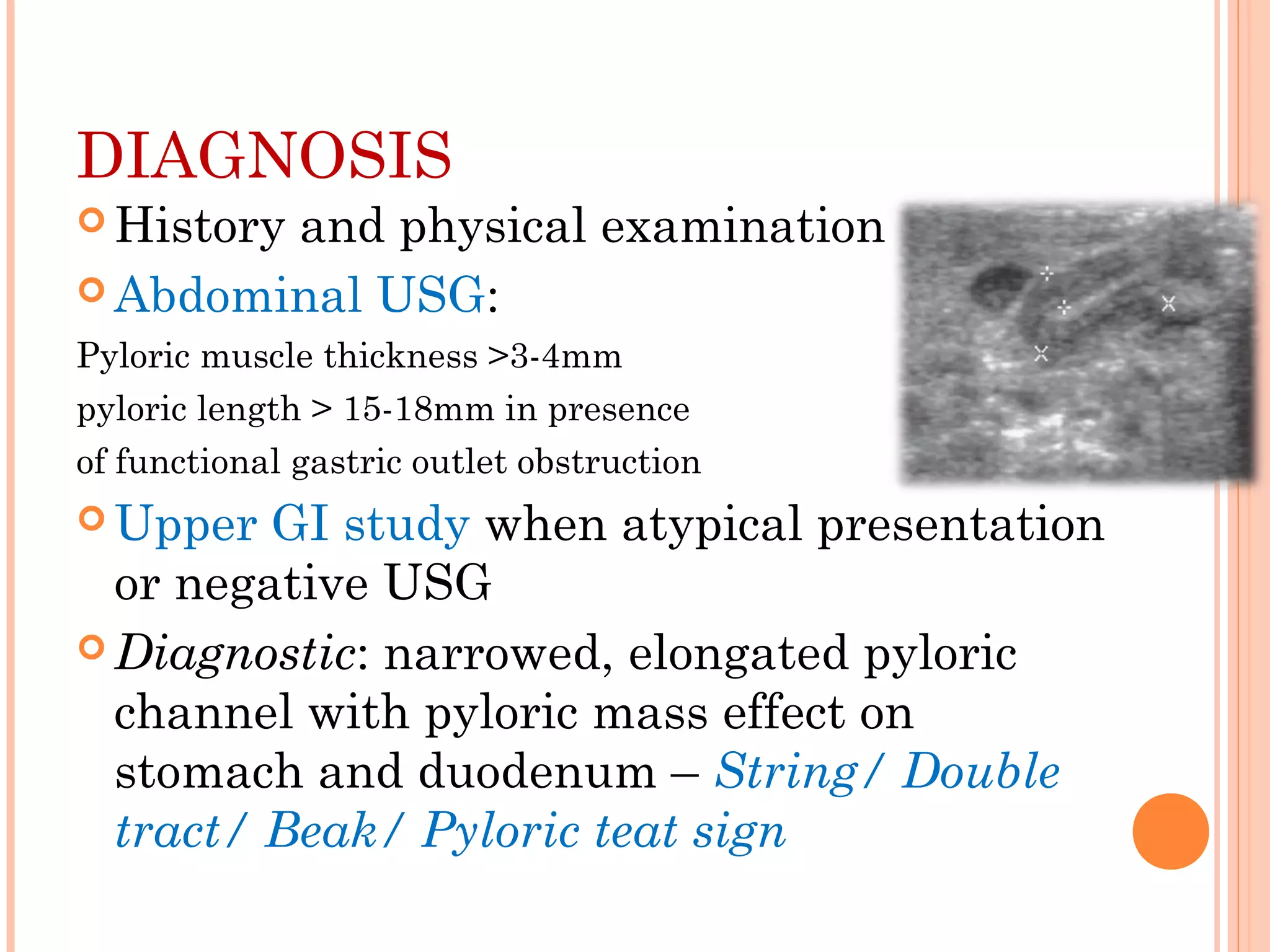
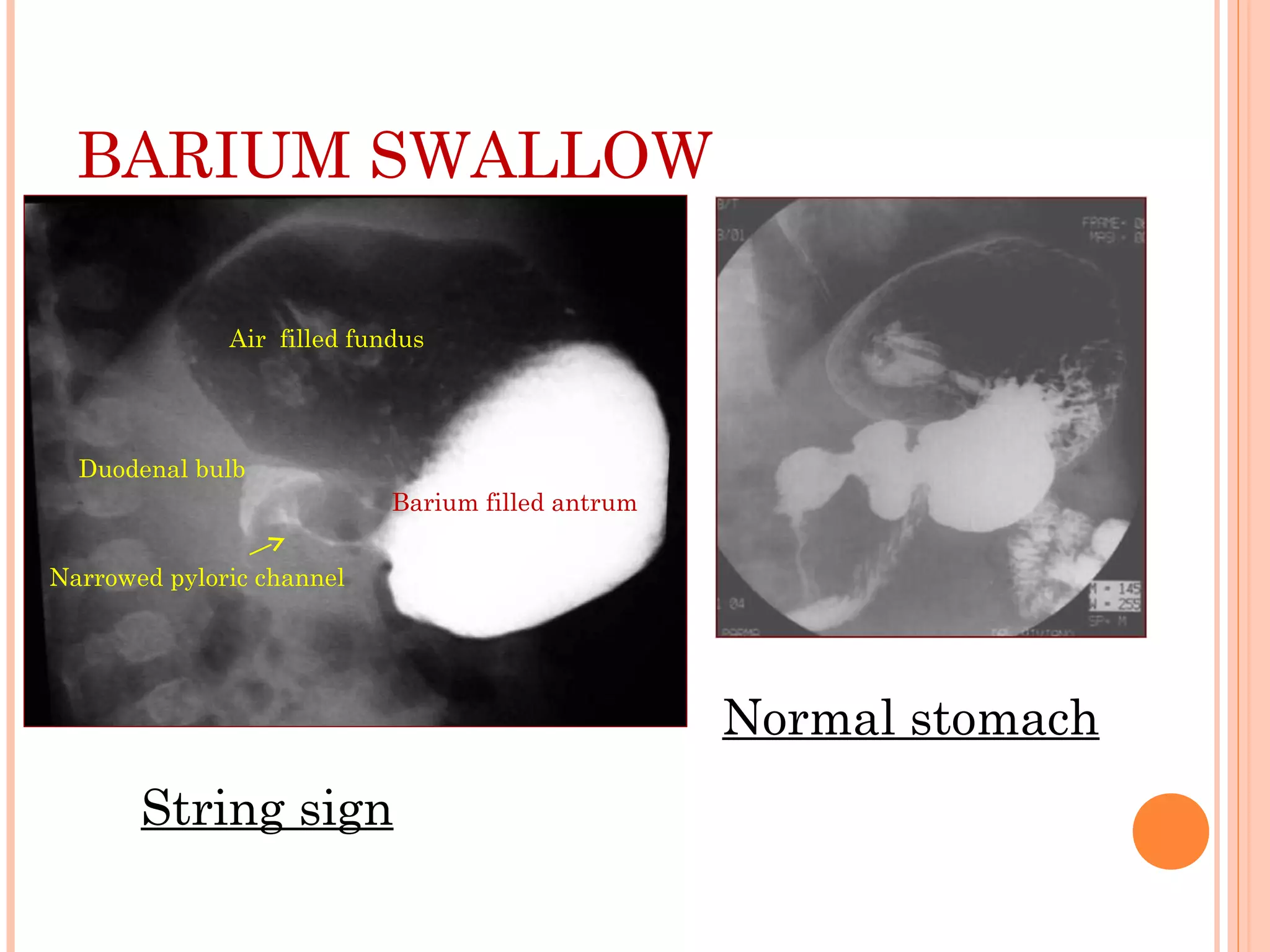









This document discusses congenital hypertrophic pyloric stenosis (CHPS), a condition where the pyloric muscle thickens, obstructing food passage from stomach to small intestine. It affects young infants, more commonly males. Presentation includes projectile vomiting after feeding. Diagnosis involves abdominal ultrasound and upper GI study. Treatment is pyloromyotomy surgery to cut the thickened pyloric muscle. The document covers epidemiology, clinical features, diagnosis, treatment including surgical procedure and postoperative care of CHPS.

































































![PYLORIC_STENOSIS IN SICK CHILDREN[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pyloricstenosisinchildren1-240909081844-b3459eee-thumbnail.jpg?width=640&height=640&fit=bounds)









































