Hypertrophic Pyloric Stenosis
•
0 likes•1,977 views

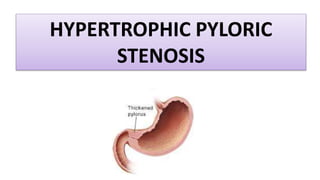
This document discusses hypertrophic pyloric stenosis, a condition where the pylorus (lower part of the stomach) becomes narrowed, preventing food from moving to the intestines. It typically affects infants 2-8 weeks old and is more common in boys. The narrowing is caused by thickening of the pyloric muscles. Symptoms include projectile vomiting and failure to gain weight. Diagnosis involves physical exam, barium X-ray, and blood tests. Treatment is pyloromyotomy surgery to open the tightened muscles. Nursing care focuses on monitoring fluids and electrolytes pre-op and the incision site and bowel function post-op.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hypertrophic Pyloric Stenosis
Similar to Hypertrophic Pyloric Stenosis (20)
More from Binand Moirangthem
More from Binand Moirangthem (20)
Recently uploaded
Recently uploaded (20)
Hypertrophic Pyloric Stenosis
- 2. DEFINITION • Narrowing and obstruction of the lower portion of stomach (pylorus) that prevents food from moving from the stomach of the intestine. • It is caused due to hypertrophy and hyperplasia of the muscles of stomach.
- 3. INCIDENCE • Typically occurs in infants between 2 – 8 weeks of age. • Affects 1 out of every 500 to 1000 live births. • More common in boys than girls.
- 4. Hypertrophy and hyperplasia of smooth muscles of pyloric sphincter Narrowing of pylorus (partial to complete obstruction) Stomach content cannot flow easily through constricted pylorus Vigorous peristalsis Vomiting and dilated stomach musculature PATHOPHYSIOLOGY
- 5. CLINICAL MANIFESTATIONS • Regurgitation and non – bilious vomiting during or after feeding (in initial stage). • Projectile vomiting (later stages). • Weight loss or failure to gain weight. • Dehydration. • Reduced frequency and amount of stool.
- 6. DIAGNOSTIC EVALUATION • Physical examination reveals a firm, olive sized mass in the epigastrium to the right of midline. • In severely malnourished infants, epigastric distension and peristaltic waves may be seen during and after feeding.
- 7. • Barium meal X- ray reveals delayed emptying of gastric contents as well as narrowing of pylorus. • Blood investigations reveals low Na, K and Cl with increased pH. • Urine examination shows concentrated urine with increased specific gravity. DIAGNOSTIC EVALUATION
- 8. MANAGEMENT
- 9. SURGICAL MANAGEMENT • Initially IV fluids are given to treat dehydration and restore the body’s normal chemistry. • After that pyloromyotomy surgery is performed. • It involves opening of tight circular muscles of pylorus that had caused narrowing. • Can be performed using either an open or laproscopic surgical approach.
- 11. PRE OPERATIVE MANAGEMENT • Monitor vital signs to detect alkalosis and fluid / electrolyte imbalance. • Note and record the amount and characteristic of vomitus and stool. • Stop oral feeding • Administer IV fluids • In partial obstruction, feed the infant in semi upright position.
- 12. • Weigh infant daily • Maintain strict intake and output chart. • Gastric lavage with normal saline before surgery. • Correct fluid and electrolyte imbalance. PRE OPERATIVE MANAGEMENT
- 13. POST OPERATIVE MANAGEMENT • Observe the incision site for drainage, signs of infection. • Keep the incision site clean and dry. • Use aseptic techniques while dressing. • Monitor abdominal girth to detect abdominal distension. • Provide calm and restful environment. • Administer IV fluids. • Assess for return of bowel sounds.
Editor's Notes
- Hypochloremic, hypokalemic metabolic alkalosis is the classic electrolyte and acid-base imbalance of pyloric stenosis. Persistent emesis causes progressive loss of fluids rich in hydrochloric acid, which causes the kidneys to retain hydrogen ions in favor of potassium.