Download to read offline

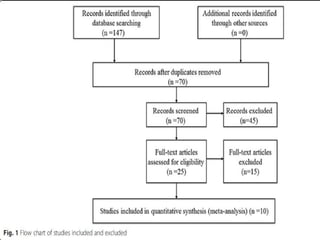
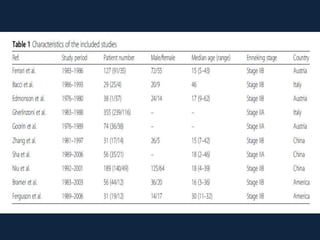
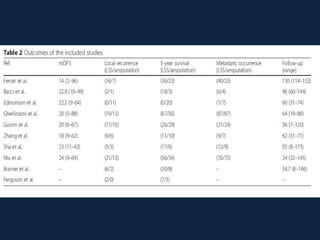
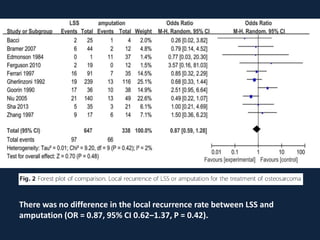
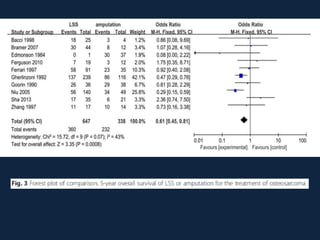
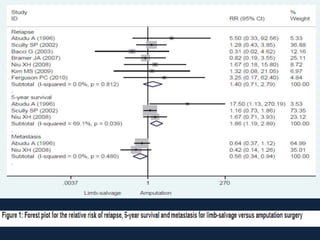
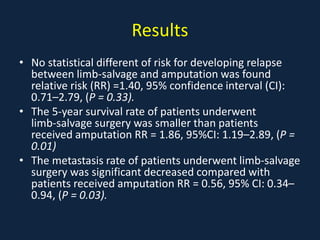





This meta-analysis examined outcomes of limb-salvage surgery (LSS) versus amputation for osteosarcoma. It found: 1) LSS had better functional outcomes than amputation. 2) The 5-year overall survival rate was higher for patients who received LSS than amputation. 3) There was no significant difference in local recurrence rates between LSS and amputation.






































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















