Presentation1, radiological imaging of hypertrophic pyloric stenosis.
•Download as PPTX, PDF•
49 likes•12,979 views

Ultrasonography is the preferred imaging method for diagnosing hypertrophic pyloric stenosis. Key findings on ultrasound include thickening of the pyloric muscle greater than 3mm and elongation of the pyloric channel greater than 17mm. Doppler ultrasound can also detect increased blood flow to the hypertrophied pyloric muscle and mucosa. While upper gastrointestinal studies with barium can identify signs like double tracking, ultrasonography has greater sensitivity and specificity for diagnosing hypertrophic pyloric stenosis.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1, radiological imaging of hypertrophic pyloric stenosis.
Similar to Presentation1, radiological imaging of hypertrophic pyloric stenosis. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of hypertrophic pyloric stenosis.
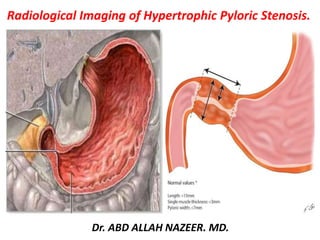
- 1. Radiological Imaging of Hypertrophic Pyloric Stenosis. Dr. ABD ALLAH NAZEER. MD.
- 2. Hypertrophic pyloric stenosis (HPS) refers to idiopathic thickening of gastric pyloric musculature which then results in progressive gastric outlet obstruction. Epidemiology Pyloric stenosis is relatively common and has a male predilection (M:F ~4:1), and is more commonly seen in Caucasians . It typically occurs between first week to 3 months of age. There may be a positive family history. Incidence of hypertrophic pyloric stenosis is approximately 2-5 per 1,000 births per year in most white populations. HPS is less common in India and among black and other Asian populations. Clinical presentation Clinical presentation is typically with non-bilious projectile vomiting. The hypertrophied pylorus can be palpated as an olive sized mass in the right upper quadrant. A succession splash may be audible, and although common, is only relevant if heard hours after the last meal. Risk factors maternal history of pyloric stenosis
- 3. Pathology HPS is the result of both hyperplasia and hypertrophy of the pyloric circular muscles fibers. The pathogenesis of this is not understood. There are four main theories: immunohistochemical abnormalities genetic abnormalities infectious cause hyperacidity theory Associations Turner syndrome Tracheo-esophageal fistula esophageal atresia trisomy 18
- 4. Radiological imaging: Radiography Abdominal radiographs may show a fluid-filled or air-distended stomach, suggesting the presence of gastric outlet obstruction. A markedly dilated stomach with exaggerated incisura (caterpillar sign) may be seen, which represents increased gastric peristalsis in these patients (see the image below). This peristaltic wave may be seen on visual inspection of the abdomen. If the patient has recently vomited or has a nasogastric tube in place, the stomach is decompressed and the radiographic findings are normal An UGI study was once considered the test of choice for hypertrophic pyloric stenosis. Findings on UGI studies include the following: Delayed gastric emptying (if severe, this may prevent barium from passing into the pylorus and severely limit the study) Cephalic orientation of the pylorus Shouldering (i.e., filling defect at the antrum created by prolapse of the hypertrophic muscle) Mushroom or umbrella sign (i.e., thickened muscle that indents the duodenal bulb; the name refers to the impression made by the hypertrophic pylorus on the duodenum) Double-track sign (i.e., redundant mucosa in the narrowed pyloric lumen, which results in separation of the barium column into 2 channels). Pyloric teat (i.e., outpouching created by distortion of the lesser curve by the hypertrophied muscle) Retained secretions and retrograde peristalsis Plain film radiography provides a low degree of confidence in making the diagnosis of or in ruling out hypertrophic pyloric stenosis. A UGI study has high sensitivity (>90%) and low specificity. High intestinal obstruction can be seen with midgut volvulus, duodenal obstruction (from stenosis, duodenal web, annular pancreas), gastric outlet obstruction caused by focal foveolar hyperplasia, and eosinophilic gastroenteritis, among others. False-negative radiographs can be seen in a child who has recently vomited.
- 5. Ultrasonography Ultrasonography is important in the diagnosis of hypertrophic pyloric stenosis and has likely contributed to the changing face of the disease, because this modality results in earlier diagnosis and treatment owing to the accessibility and accuracy of ultrasonography.This modality is the method of choice for both the diagnosis and exclusion of hypertrophic pyloric stenosis, because ultrasonography has a sensitivity and specificity of approximately 100%.Thus, ultrasonography is also recommended in patients whose disease is clinically suspected but in whom the pyloric olive cannot be felt. In a study by Leaphart et al, ultrasonography confirmed hypertrophic pyloric stenosis when the pyloric muscle thickness (MT) was greater than 4 mm and the pyloric channel length (CL) was greater than 15 mm. The investigators studied the diagnostic criteria for this disease in newborns younger than 21 days from 2000 to 2006 and found that ultrasonographic measurement of hypertrophic pyloric stenosis was significantly decreased in younger patients (MT, 3.7 +/- 0.65 mm; CL, 16.9 +/- 2.8 mm) versus older newborns (MT, 4.6 +/- 0.82 mm; CL, 18.2 +/- 3.4 mm). Of important note, the mean ultrasonographic measurement for young newborns with hypertrophic pyloric stenosis typically fell within the range currently defined as normal or borderline.A linear relationship existed between pyloric MT and CL and patient age, suggesting that 3.5 mm MT be considered the cutoff in younger patients.
- 6. Technique Ultrasonography is performed with a 7.5- to 13.5-MHz linear transducer in the supine child. Transverse images at the epigastrium identify the pylorus to the left of the gallbladder and anteromedial to the right kidney (see the image below). A distended stomach, however, displaces and distorts the pylorus and may require the placement of a nasogastric tube to withdraw the stomach's contents. A gastric aspirate of more than 5 mL in a baby who has been without oral intake (NPO) for several hours indicates gastric outlet obstruction. Right posterior oblique positioning and scanning from a posterior approach may help to improve visualization of the pylorus. Ultrasonographic signs of hypertrophic pyloric stenosis, originally described in 1977and further defined, are as follows: A MT (serosa to mucosa) greater than 3 mm (a correlation between MT and the patient's age exists; the most reliable ultrasonographic sign is an MT greater than 3 mm. Because this measurement can be increased falsely with off-axis imaging, attention to technique is important.) Target sign on transverse images of the pylorus.
- 7. Pyloric channel length greater than 17 mm Pyloric thickness (serosa to serosa) of 15 mm or greater Failure of the channel to open during a minimum of 15 minutes of scanning Retrograde or hyper peristaltic contractions Antral nipple sign (i.e., a prolapse of redundant mucosa into the antrum, which creates a pseudomass Double-track sign on ultrasonography(i.e., redundant mucosa in the narrowed lumen, which creates 2 mucosal outlines) Other findings include reversible portal venous gas; nonuniform echogenicity of the pyloric muscle.
- 9. Supine radiograph in an infant with vomiting demonstrates the caterpillar sign of active gastric hyperperistalsis.
- 10. Lateral view from an upper gastrointestinal study demonstrates the double-track sign.
- 11. Upper gastrointestinal study from a child shows the string sign (see inset).
- 13. Stomach shows double tracking in region of pyloric canal, indentation on base of bulb and delayed gastric emptying.
- 14. Fluoroscopic image from UGI in a patient with IHPS. Contrast material courses through the mucosal interstices of the canal, forming the double-track sign (large arrowheads), with an additional central channel along the distal portion (small arrowhead). Mass impression on the gastric antrum (arrow), best seen during peristaltic activity, is termed the shoulder sign.
- 15. TYPICAL UPPER GASTROINTESTINAL SERIAL IN A 2 YEARS OLD BOY WITH HYPERTROPHIC PYLORIC STENOSIS. Narrowing of pyloric canal pushes hypertrophic pylorus upwards and posteriorly to the duodenal bulb impressing the lesser curvature of the stomach. All of that results as the "beak sign" and "tit sign" respectively.
- 16. HYPERTROPHIC PYLORIC STENOIS IN A 2 YEARS OLD BOY. Plain radiograph shows severe distension of the stomach with air-fluid level inside due to complete outlet stop. Lateral view on barium exam shows narrowing and elongation of pyloric canal as well as stretching of the duodenal bulb due to hypertrophied pylorus. Notice as ell, the existence of the “string sign” or the “double track sign”.
- 17. Double-track sign - Contrast studies showing redundant mucosa separates barium into two columns in pyloric channel.
- 18. Tit sign - contrast study showing an outpouching created on lesser curve by distorted muscle in hypertrophic pyloric stenosis.
- 19. INFANTILE HYPERTROPHIC PYLORIC STENOSIS.
- 20. Hypertrophic pyloric stenosis demonstrates the target sign and heterogeneous echo texture of the muscular layer (the pylorus is deep to the anechoic gallbladder).
- 21. The distended stomach (*), posteriorly displacing the pylorus (arrow), which resembles the appearance of the uterine cervix, of congenital pyloric stenosis.
- 22. The hypertrophied muscular layer. Abnormal elongation of the pyloric canal (measure 1)
- 23. Infantile Hypertrophic Pyloric stenosis.
- 24. Infantile Hypertrophic Pyloric stenosis
- 25. Infantile Hypertrophic Pyloric stenosis.
- 26. a. Sonograms in a patient with IHPS. (a) Longitudinal sonogram shows anterior thickened muscle (cursors). Double layer of crowded and redundant mucosa fills the channel and protrudes into fluid-filled antrum (arrow). D = fluid-filled duodenal cap. (b) Cross-sectional sonogram shows circumferential muscular thickening (cursors) surrounding the central channel and filled with mucosa (M).
- 27. Longitudinal sonograms obtained within a few minutes of each other show peristaltic activity and changes in pyloric anatomy in a patient with IHPS. Note the shorter canal in image on left and subsequent elongation coincident with peristaltic activity in image on right. There is failure of relaxation of the pyloric channel, and persistent obliteration of the lumen. Also note that on the left image, the gastric contents and pyloric mucosa have similar echogenicity, falsely suggestive of unimpeded passage of gastric contents through the canal. A = antrum, D = duodenal cap, arrows = outer muscular layer.
- 28. a The double layer of thickened mucosa (*), b protruding through the antrum
- 29. Peristaltic changes in antropyloric anatomy on normal sonographic study. Left: Antropyloric channel is closed during peristaltic activity. Right: Distal antrum (A) is fully relaxed. Arrows = pyloric ring, D = duodenal cap.
- 30. Sonographic measurement of pylorus canal length (Cervix sign in IHPS). Color Doppler Examination of the pylorus showing vascularity in the mucosa s& pyloric muscle.
- 31. 1a. Longitudinal plane showing the elongated pylorus with thickened pyloric muscle. 1b. Transverse plane showing ‘target sign’ with thickened pyloric muscle.
- 32. In longitudinal plane the pyloric canal length is 18mm, The pyloric muscle thickness measuring 4.6 mm and the pyloric diameter measuring 14 mm.
- 33. The ultrasound imaging showing the "donut" lesion. The ultrasound imaging showing the increase of the longitudinal length measure (16,9 mm) and an increase in the thickness of the pyloric muscular wall (11,9 mm).
- 34. Axial oblique ultrasound shows thickened, hypoechoic muscular wall (5.4 mm) and elongated pyloric canal (17.2 mm approximately).
- 35. The pyloric channel appears significantly elongated and the thickened, hypoechoic muscular layers are well appreciated. The pyloric lumen is reduced and the apposed echogenic mucosal layers of both sides are noted. The axial images demonstrate target sign.
- 37. Thickening of pyloric wall is seen. Single wall thickness is 4-5 mm (normal is up to 3 mm). Length of pyloric canal is 18-20 mm (normal is up to 16 mm).
- 38. Doppler US findings in patients with IHPS. (a) Longitudinal image shows markedly increased flow to hypertrophied pylorus in 4-week-old girl. Solid arrows point to muscle layer. Open arrow points to mucosal flow. (b) Transverse image obtained in 5-week-old girl. Note the collar of increased flow in the submucosal plexus, branching into the luminal mucosa and adjacent muscle layer (arrows). (c) Longitudinal image of hypertrophied pylorus in 3-week-old boy with typical IHPS. Note the increased flow to the mucosa within the canal, protruding into the adjacent fluid-filled antrum (A).Straight arrows outline the adjacent thickened muscle. Curved arrow points to base of duodenal bulb. (d) Longitudinal image of hypertrophied pylorus in 5-week-old boy with typical IHPS. Note the markedly increased flow to the mucosal layer, which is detailed in the spectral tracing at the bottom of the image. A = antrum. (e) Longitudinal image of hypertrophied pylorus in 2-week-old boy with IHPS. Note the markedly increased flow to the muscle layer, which is detailed in the spectral tracing at the bottom of the image. D = duodenal bulb. (f) Longitudinal image of atypical pylorus in 5-week-old boy with IHPS. Although there is detectable flow, it is less visible than that in most other patients with IHPS. Arrows point to muscle layer. (g) Transverse image of pylorus in same patient as in f, with similar findings. Arrows point to muscle layer.
- 39. Doppler US findings in patients without IHPS (control patients). A = antrum, D = duodenal bulb. Longitudinal images obtained in (a) a 2-month-old boy, (b) a 3-month-old boy, and (c) an 8-week-old girl show no detectable flow. Antropyloric canal is closed in a and open in b and c. (d) Longitudinal image obtained in 10-day-old girl shows atypical high flow in the open antropyloric canal. There is visible flow to the dorsal portion of the muscle layer.
- 40. Thank You.