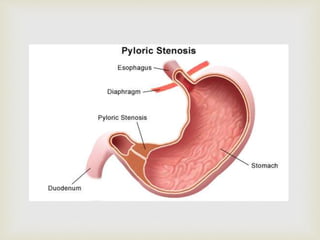
This document discusses infantile hypertrophic pyloric stenosis (IHPS), a condition where the pyloric muscle of the stomach becomes thickened, preventing food from passing normally into the small intestine. The key points are:
- IHPS is most common in firstborn males under 6 weeks of age and may be linked to erythromycin use as an infant.
- Symptoms include projectile vomiting, dehydration, and weight loss. Diagnosis involves feeling an olive-sized lump in the stomach and confirming on ultrasound or blood tests.
- Treatment involves rehydration followed by pyloromyotomy surgery to cut the thickened muscle and allow food to pass through. Complications