
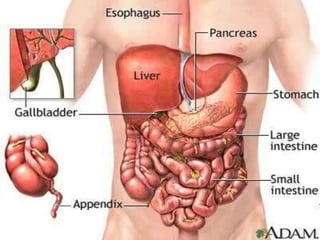
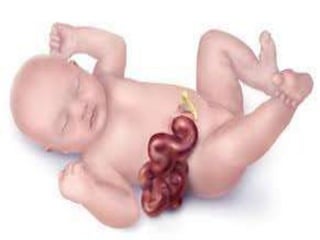
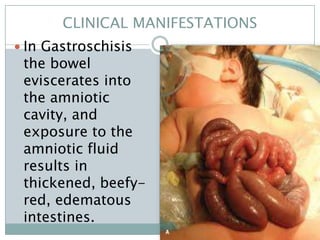
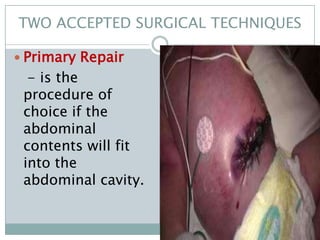
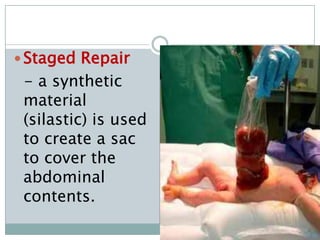

Gastroschisis is a birth defect where a hole in the abdominal wall allows intestines to protrude outside the baby's body. It occurs in about 0.1-0.3% of live births. The defect is usually on the right side of the belly button, with no protective sac covering the intestines. Treatment involves surgery to return the intestines to the abdominal cavity. Nursing care focuses on keeping the exposed intestines warm and sterile, managing fluids and nutrition, and monitoring for complications like infection or obstruction. Primary repair is preferred if the intestines will fit back inside, otherwise a staged repair using a synthetic sac is required.
























































![Neonatal nursing care for GZIT[Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/ambayenntwoassigmentautosaved-231228091237-bb9a1ff0-thumbnail.jpg?width=640&height=640&fit=bounds)










