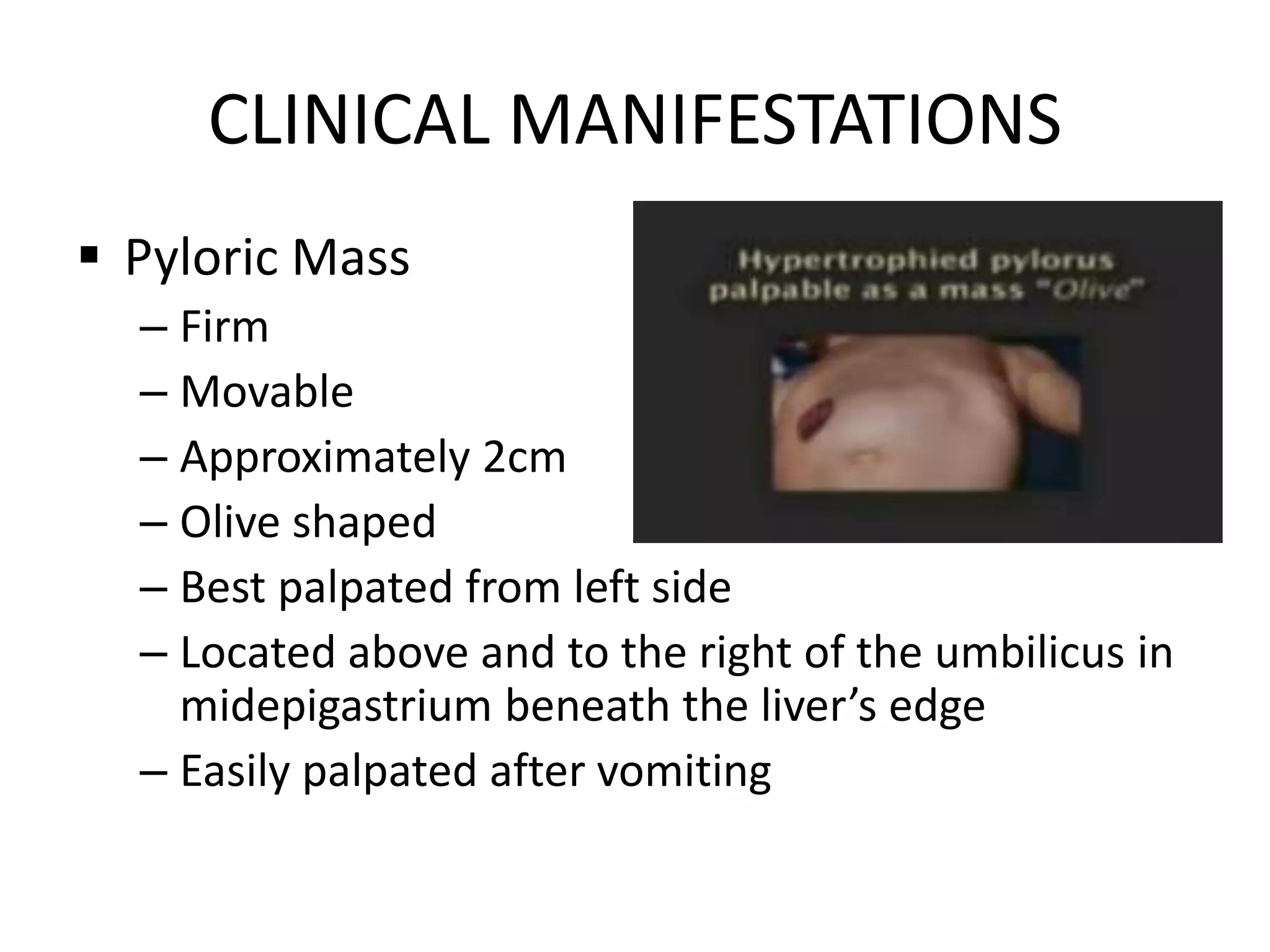
Kelly, a 6-month old infant, has been vomiting whenever she is fed for the past 2 weeks. Her parents noticed an olive-shaped mass in her abdomen. They took her to their local pediatrician. The pediatrician suspects Kelly may have hypertrophic pyloric stenosis based on her symptoms of vomiting after feeding and the presence of a pyloric mass.