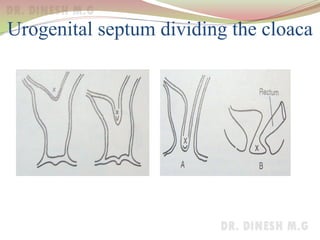
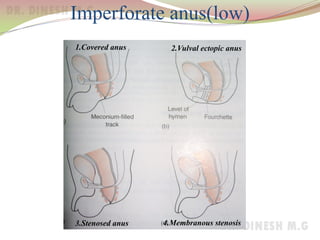
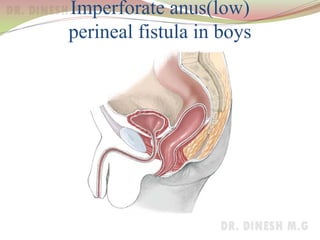
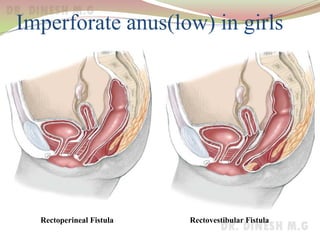
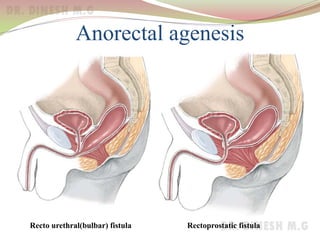
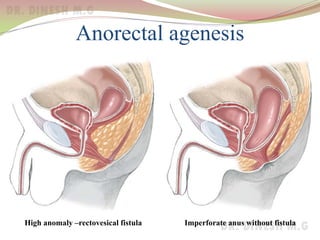
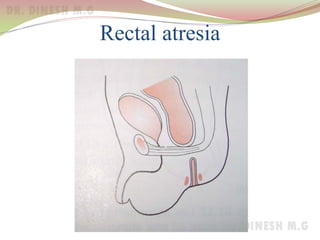
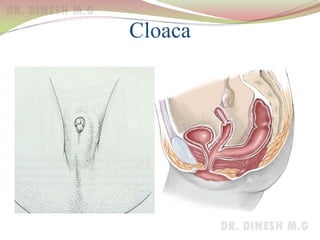
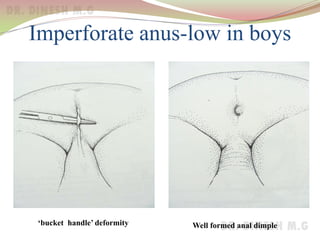
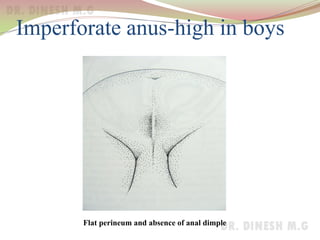
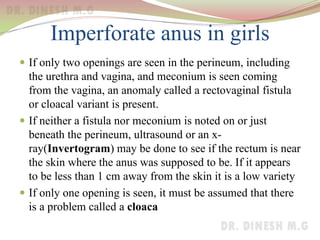
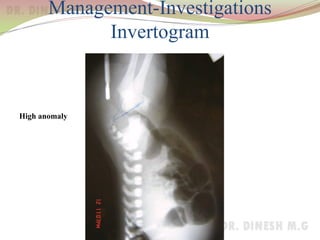
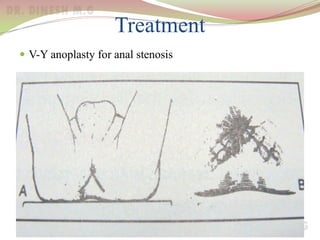
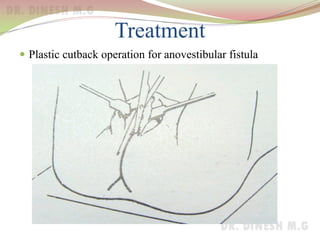
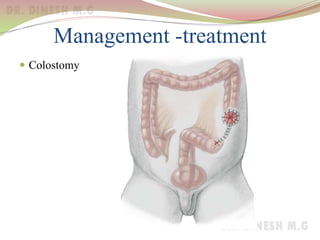
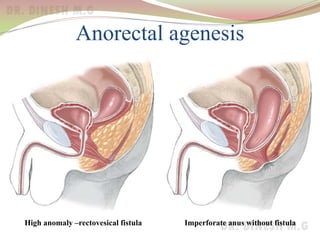
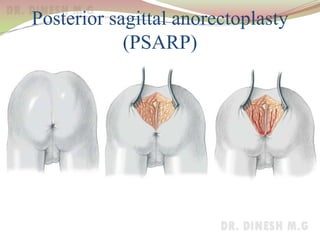
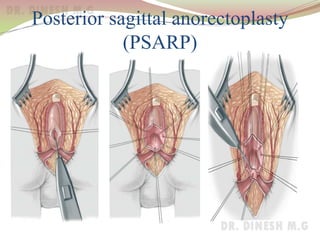
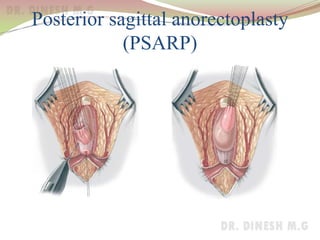
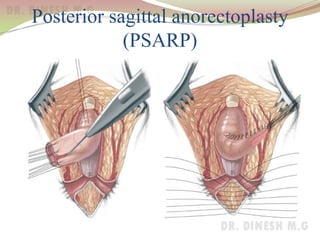
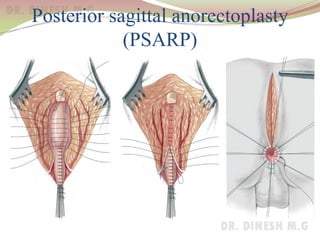
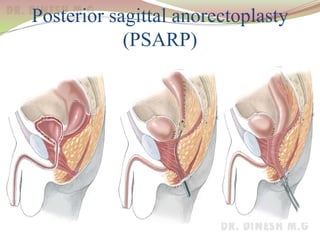




The document discusses the development of the anal canal and the surgical anatomy of the anal canal. It describes different types of imperforate anus including low and high anomalies. Low anomalies include covered anus, ectopic anus, and stenosed anus. High anomalies include anorectal agenesis, rectal atresia, and cloaca. Initial management involves assessing whether temporary colostomy is needed. Treatment of low anomalies involves dilatations or procedures like V-Y anoplasty or cutback procedure. Treatment of high anomalies includes initial colostomy followed by posterior sagittal anorectoplasty to reconstruct the anal canal. Surgical outcomes vary depending on the type of anomaly repaired.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

