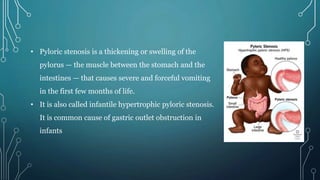
1. Pyloric stenosis is a condition where the pylorus, the muscle between the stomach and intestines, thickens and causes projectile vomiting in infants. It commonly affects baby boys in their first few months.
2. Congenital gastric outlet obstruction is a rare birth defect that blocks or narrows the passage from the stomach to the intestines, preventing food from passing through. It can cause vomiting, poor weight gain, and dehydration.
3. Both conditions require surgery to correct the obstruction - for pyloric stenosis, a pyloromyotomy to cut the thickened muscle. With prompt treatment, infants generally recover well without long-term issues.