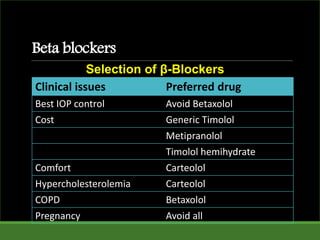
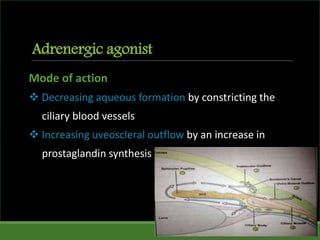
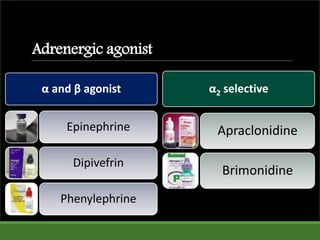
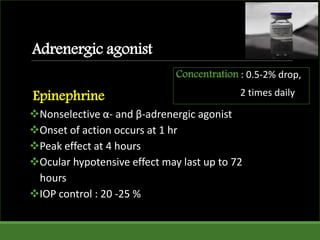

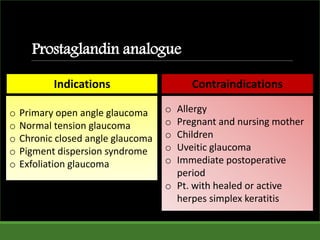
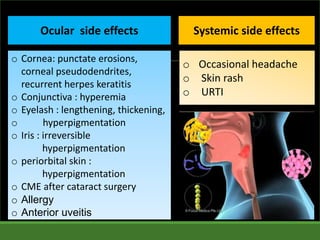



The document is a comprehensive presentation on anti-glaucoma drugs, detailing their classification, mechanisms, indications, and contraindications. It covers various drug categories like beta-blockers, adrenergic agonists, cholinergic agents, and prostaglandin analogues, discussing specific medications, their efficacy, side effects, and the therapeutic goal of lowering intraocular pressure to manage glaucoma. The document serves as a guideline for prescribing these medications to optimize patient treatment and minimize side effects.




































































































