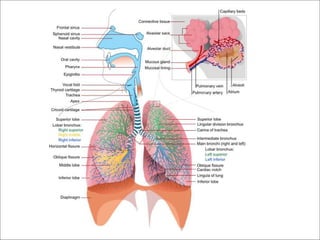

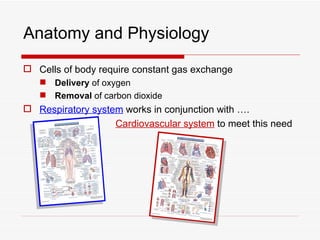
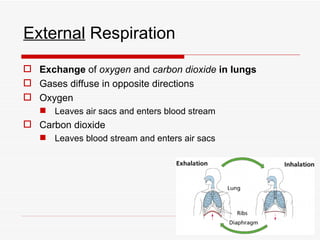
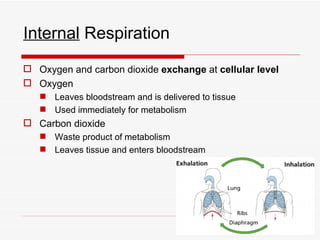
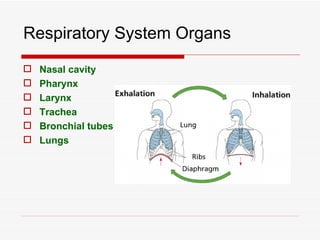
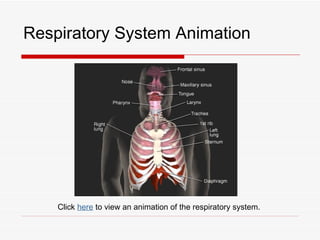
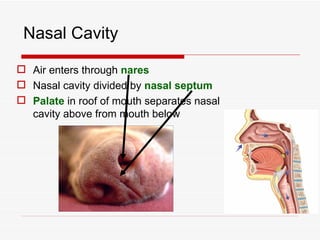
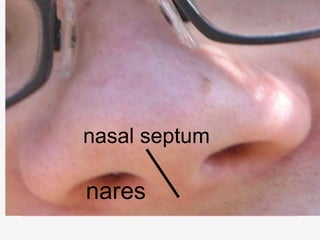
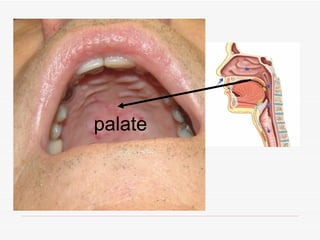
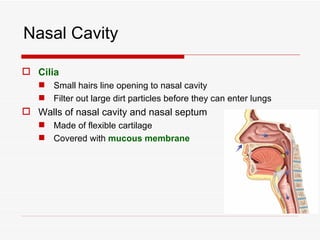
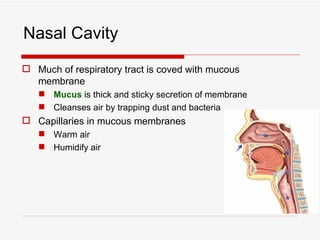
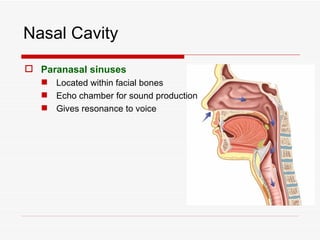
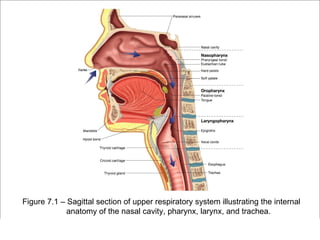
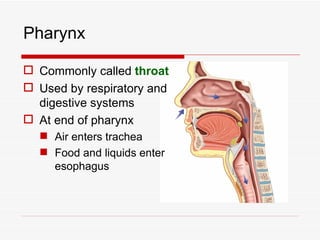
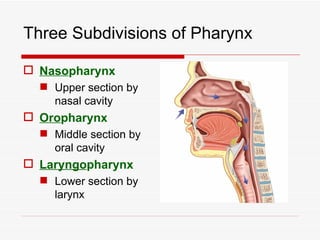
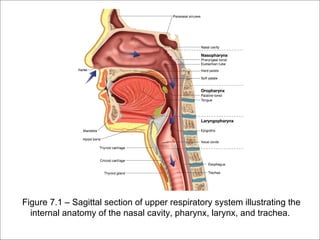
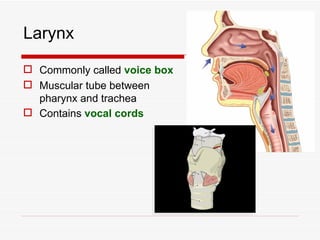
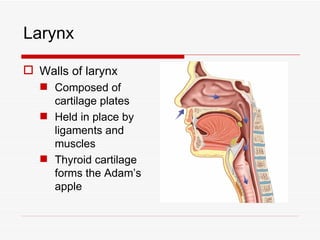
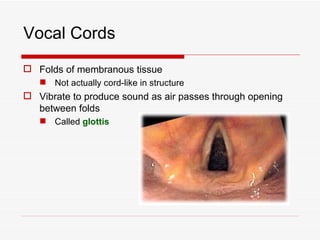
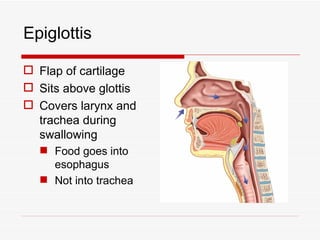
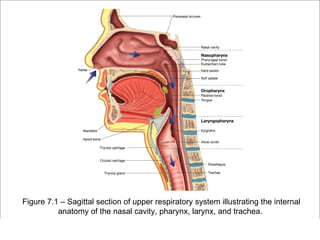
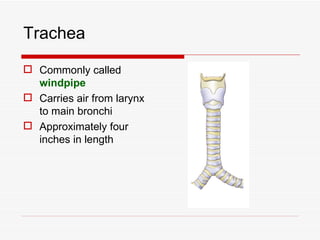
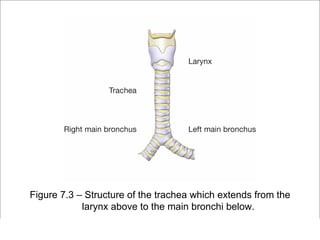
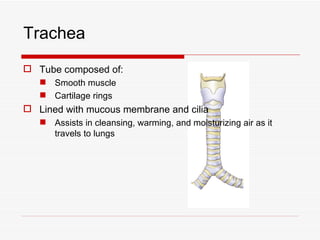
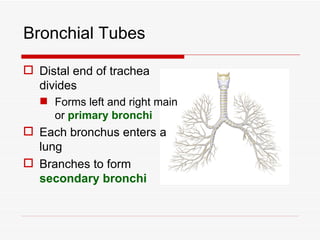
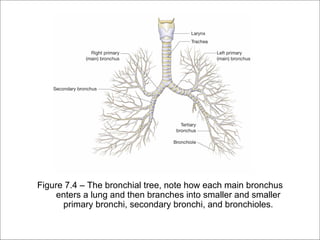
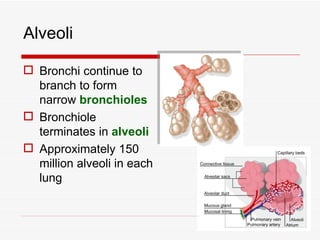
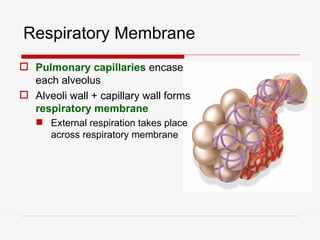
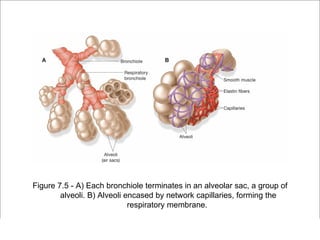
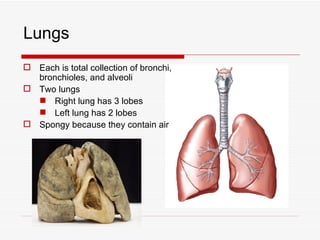

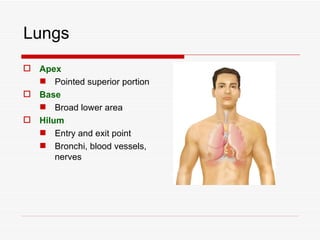
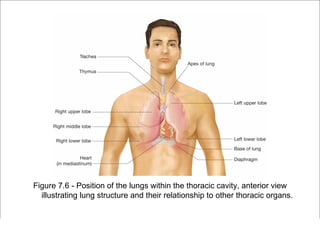
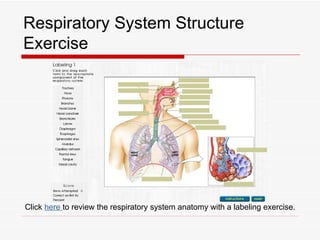

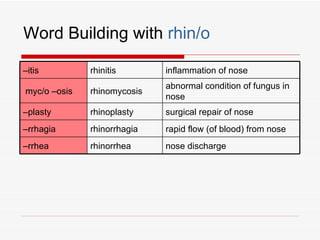
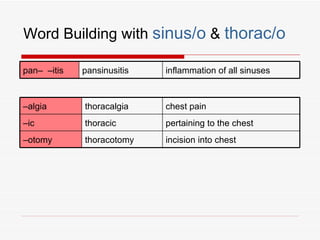
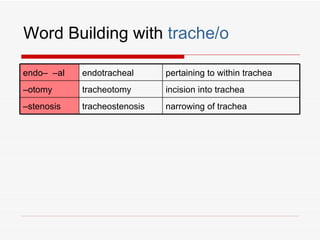
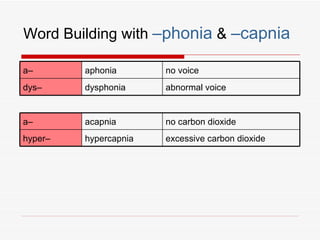

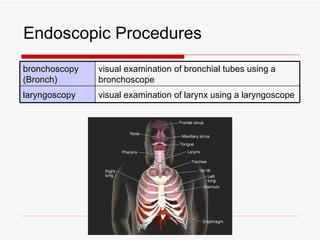


The respiratory system has several functions including inhaling oxygen and exhaling carbon dioxide. It is comprised of organs like the nasal cavity, pharynx, larynx, trachea, bronchial tubes, and lungs. The nasal cavity warms and humidifies air before it reaches the lungs. The pharynx is shared by the respiratory and digestive systems. The larynx contains the vocal cords which produce sound. The trachea transports air to the bronchi and lungs. In the lungs, bronchioles divide into alveoli where gas exchange occurs across the respiratory membrane.































































![Lesson6 [2 Oth Oct 2008]](https://cdn.slidesharecdn.com/ss_thumbnails/lesson62othoct2008-091022023449-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



































