Download as PDF, PPTX



















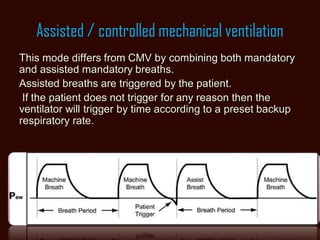



















The document explains key concepts of mechanical ventilation in an ICU setting, focusing on ventilator variables, modes, and their clinical applications. It details the five types of ventilator variables: control, trigger, limit, cycle, and baseline, as well as various breath types and ventilation modes such as CMV, A/C, SIMV, and pressure support. Finally, it discusses the advantages and disadvantages of each mode, emphasizing the importance of proper ventilator settings to ensure patient safety and comfort.























































































