Download to read offline


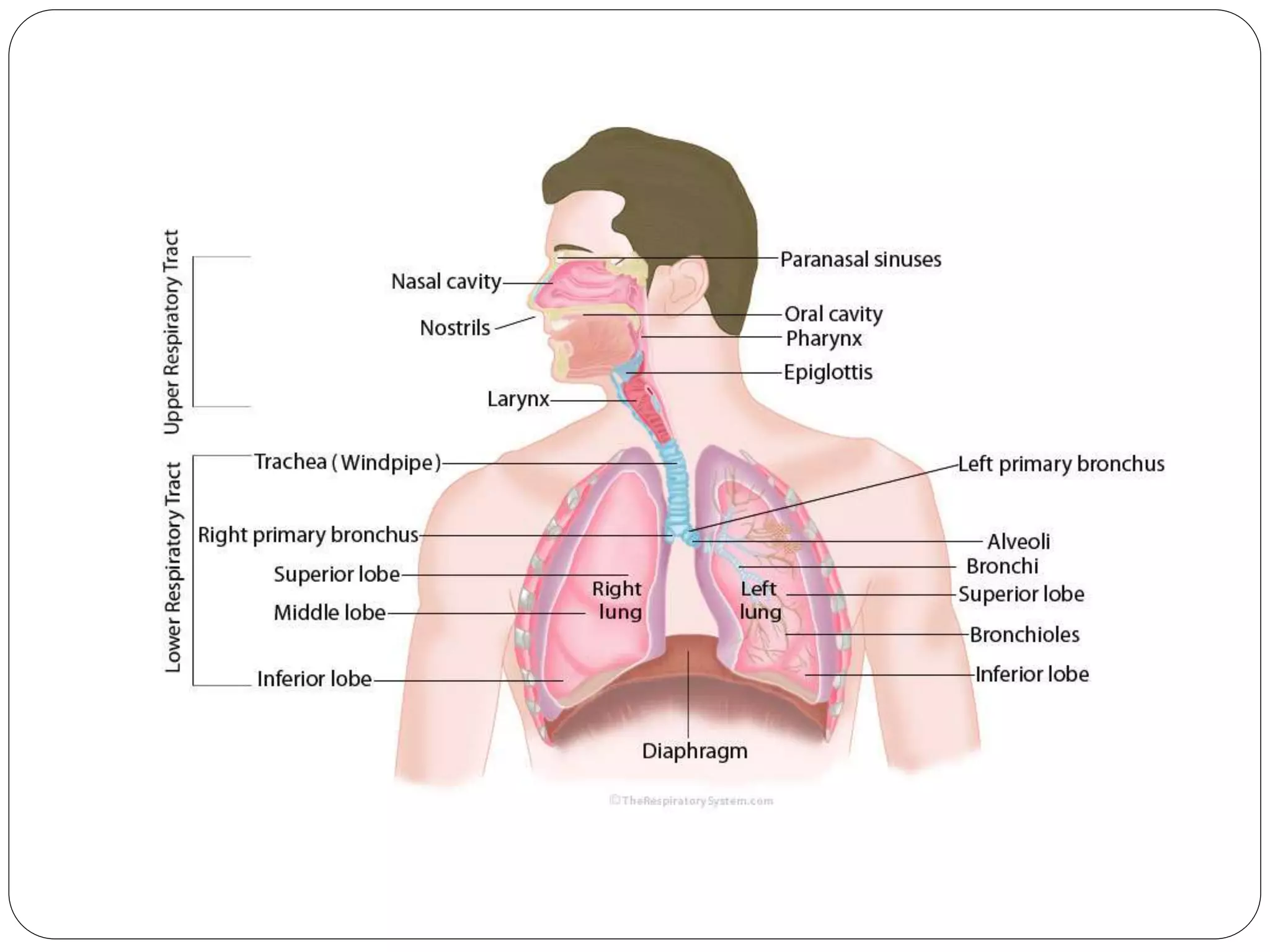







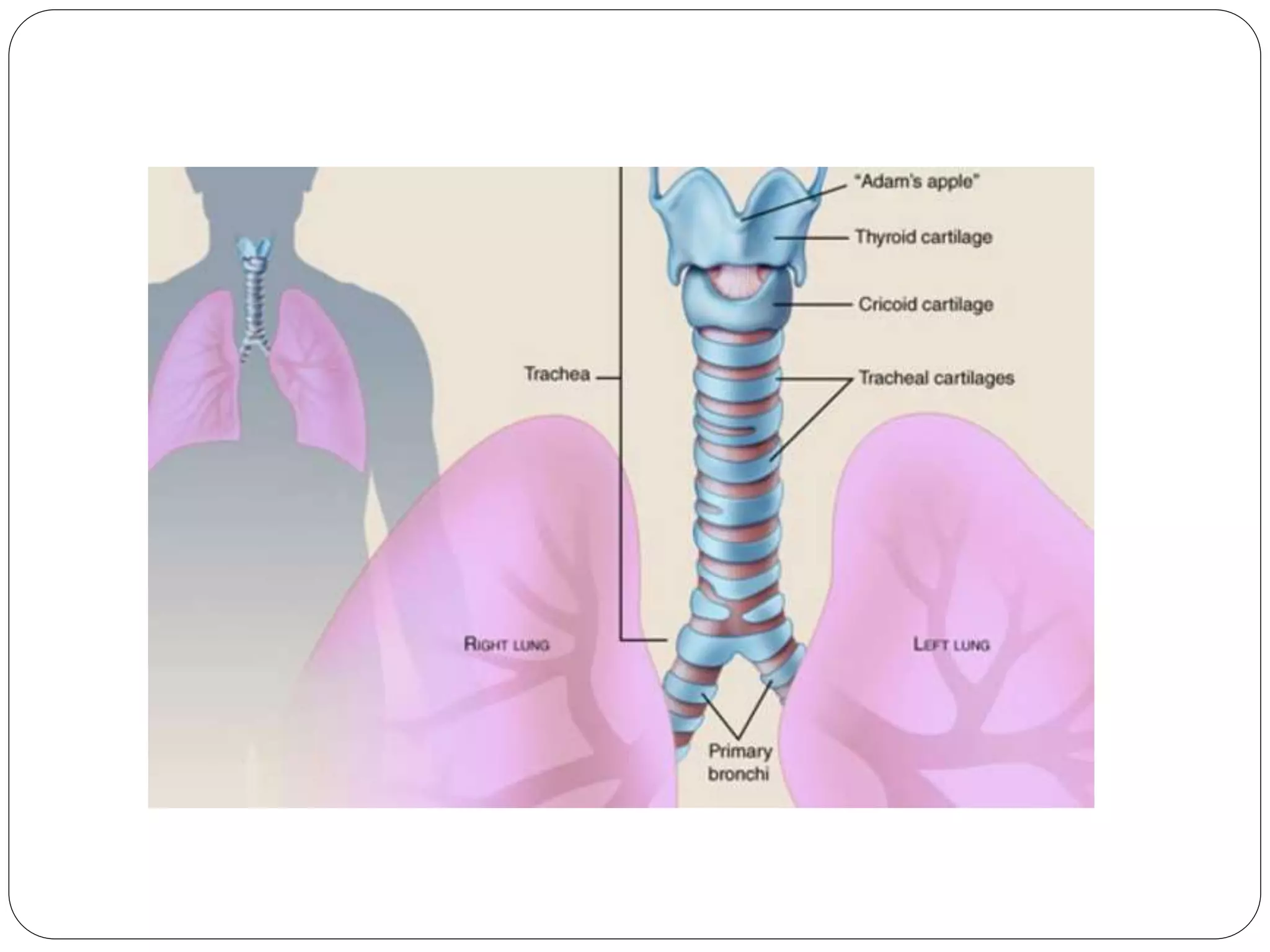











































The document presents a comprehensive overview of the respiratory system, detailing its anatomy, functions, and processes involved in respiration. It covers key components such as the upper and lower respiratory tracts, the mechanics of breathing, gas exchange, and the roles of various structures like the lungs and trachea. Additionally, it explains the physiological processes of external and internal respiration, including the transport of oxygen and carbon dioxide within the body.