Downloaded 933 times

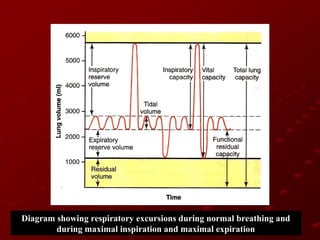

This document discusses respiratory function and its importance to anesthesia. It covers topics like cellular respiration, aerobic vs anaerobic respiration, muscles of respiration, mechanisms of ventilation, lung volumes, compliance, and factors that affect respiration. The speaker is Dr. Tipu and the event is being coordinated by Dr. Shivali Pandey.











































































































