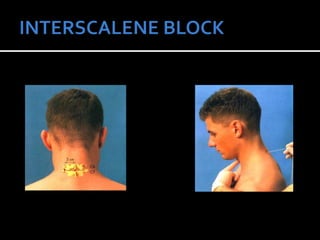
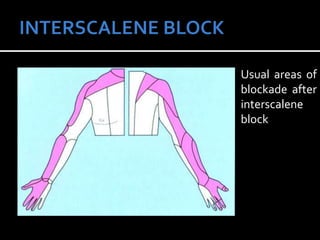
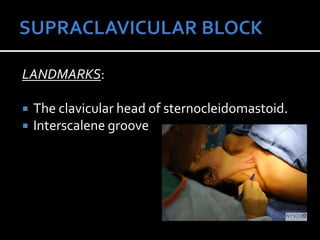
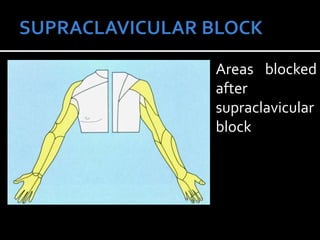
This document provides information on interscalene brachial plexus blocks, including indications, contraindications, anatomy, techniques, complications, and references. It describes Winnie's anterior approach using landmarks to identify the interscalene groove for injection, as well as a posterior approach. Areas of blockade, continuous techniques, and use of nerve stimulation are also summarized. Supraclavicular blockade as an alternative is outlined with similar details.