Downloaded 123 times
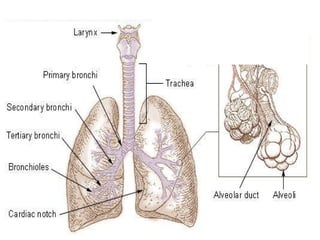













































The document discusses various aspects of respiration including external respiration in the lungs involving gas exchange, and internal respiration in the mitochondria involving oxygen utilization. It describes the conducting and respiratory zones of the lungs, pleura, pulmonary pressures, respiratory muscles, mechanisms of inspiration and expiration. It also summarizes lung compliance, surfactant, pulmonary ventilation tests, lung volumes, dead space, and pulmonary function tests.























































































