Downloaded 2,624 times

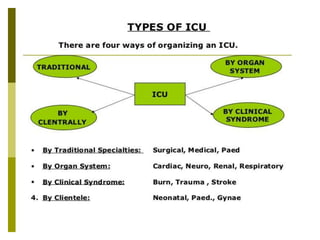

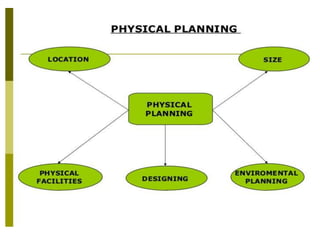
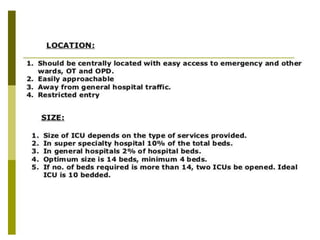
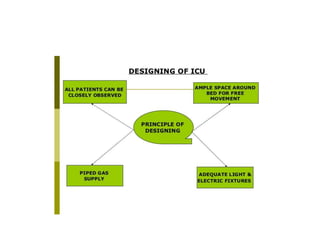


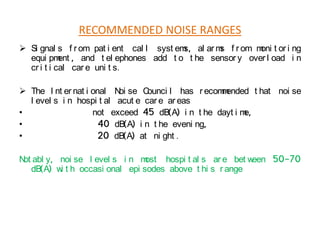





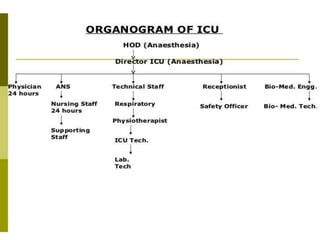


This document outlines guidelines for organizing intensive care units (ICUs) at different levels of a hospital. It discusses ICU levels I-III and their recommended features. Level I ICUs are for small hospitals and provide basic monitoring and short-term care. Level II ICUs have expanded capabilities and staff training. Level III ICUs provide the highest level of multisystem care and technology. The document also covers ICU unit design considerations, including patient area layout, noise levels, nursing stations, and necessary equipment and utilities. Staffing guidelines recommend intensivists to lead the team along with residents, nurses, respiratory therapists and other support staff tailored to the ICU's needs and capabilities.











































![4._LAY_OUT_OF_CRITICAL_CARE_UNIT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250506110215-46b0d8f2-thumbnail.jpg?width=640&height=640&fit=bounds)











































