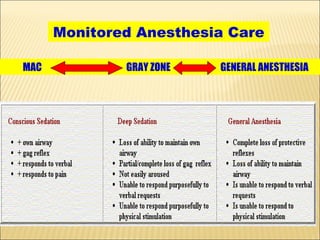
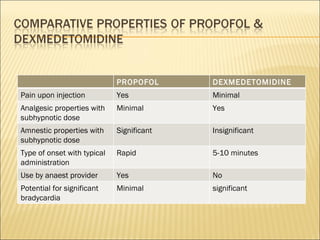
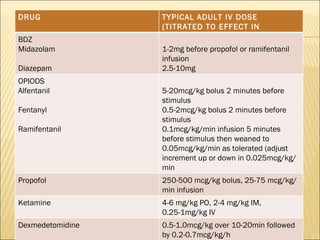
The document discusses monitored anesthesia care (MAC), which involves administering drugs to provide anxiolytic, hypnotic, amnestic, and analgesic effects without depressing consciousness below a certain level. It provides guidelines on drug selection and dosing for MAC, including opioids like fentanyl and remifentanil, benzodiazepines like midazolam, propofol, ketamine, and dexmedetomidine. It also discusses factors that can lead to patient agitation during MAC and principles of drug administration via continuous infusion or patient-controlled methods.