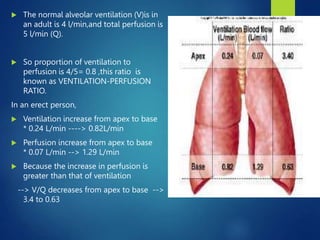
The document provides an extensive overview of respiratory physiology, highlighting the functional residual capacity (FRC), its influencing factors, and the concept of closing capacity (CC). It details ventilation-perfusion ratios and the impact of various conditions on gas exchange efficiency, as well as central and peripheral chemoreceptor roles in regulating breathing. Additionally, it discusses the effects of posture, age, and specific medical conditions on respiratory function and dead space in the lungs.

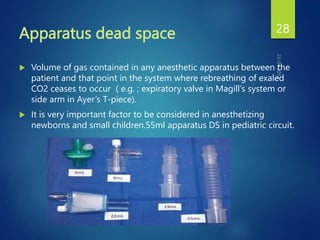
![Anatomical Dead Space
Not all of the inspired air reached the alveoli.
As fresh air is inhaled it is mixed with air in anatomical
dead space.
Conducting zone and alveoli where [02] is lower than
normal and [C02] is higher than normal.
Alveolar ventilation = F x (TV- DS).(apprx 5L).
F = frequency (breaths/min.).
TV = tidal volume.
DS = dead space.
www.freelivedoctor.com](https://image.slidesharecdn.com/respiratoryphysiology-2sanjay-240326225358-d3dc348f/85/Respiratory-Physiology-2-sanjay-pptx-good-23-320.jpg)