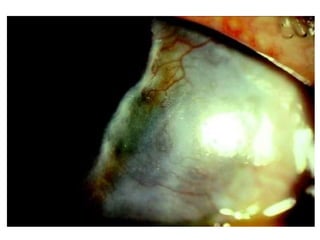
Marginal corneal ulcer, also known as Mooren's ulcer, is a rare degenerative ulcer that starts at the corneal margin and spreads circumferentially and axially over the cornea. It is a rapidly progressive and painful ulcerative keratitis that can only be diagnosed in the absence of a systemic cause. It must be differentiated from other corneal abnormalities. Benign cases are unilateral, respond well to treatment, and affect elderly people, while malignant cases are bilateral, respond poorly to treatment, and affect younger people in a progressive manner. It is considered an autoimmune disorder associated with infections and various theories about antigen-antibody reactions and molecular mimicry stimulating an autoimmune response.