Downloaded 635 times
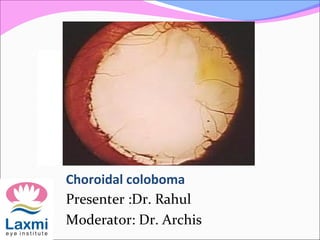
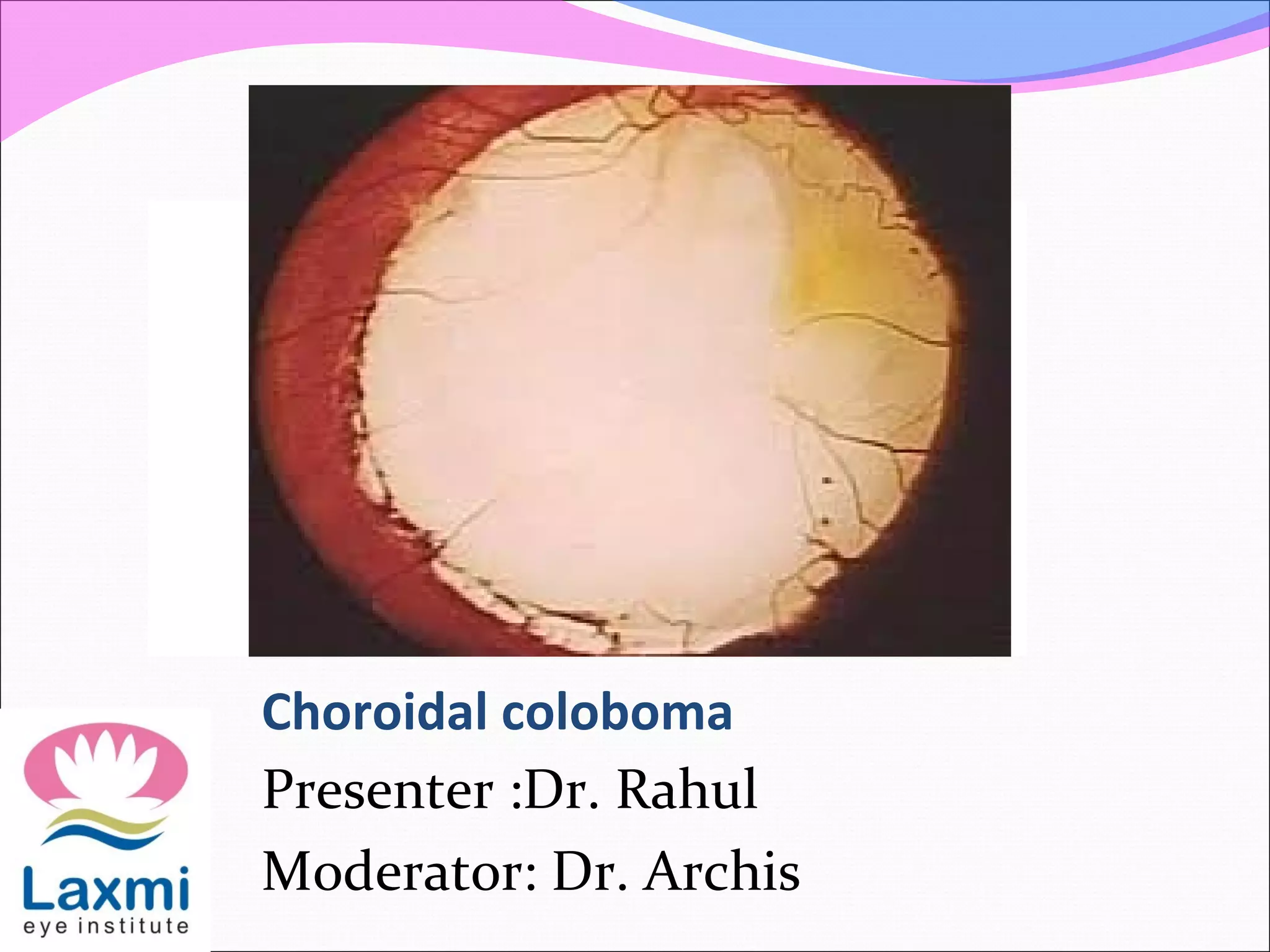
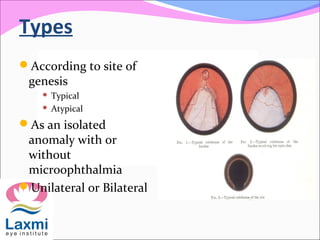
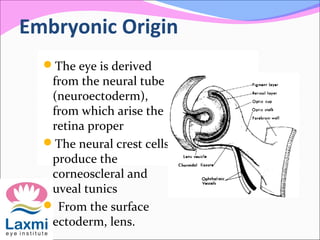
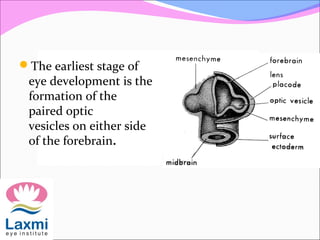
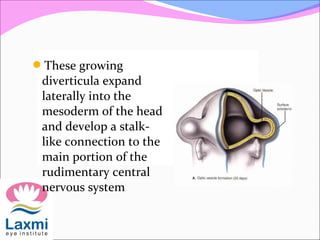
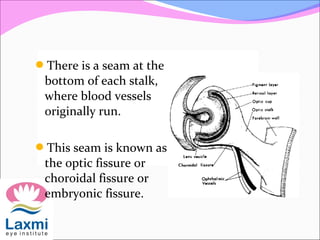


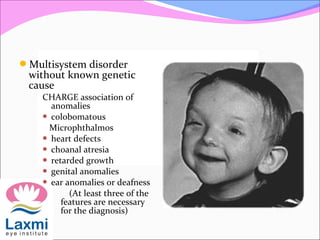
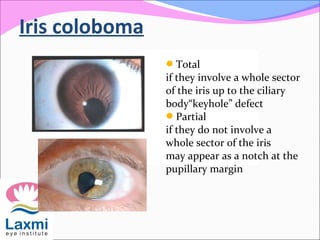
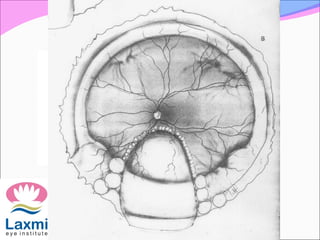


This document discusses choroidal coloboma, beginning with definitions and epidemiology. It describes the embryonic development of the eye and how failure of fusion of the embryonic fissure can result in coloboma. Types of coloboma are classified based on location and presence of other anomalies. Complications like retinal detachment are discussed. Management of cataracts and other ocular issues in the context of coloboma are covered. The prognosis depends on factors like presence of microphthalmos, corneal diameter, and type and timing of surgery.























































































