Download as PDF, PPTX


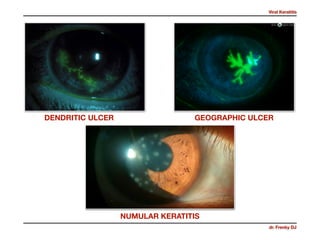
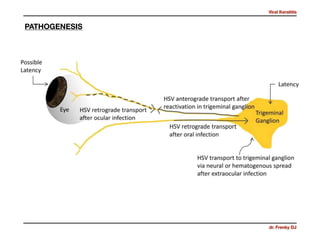

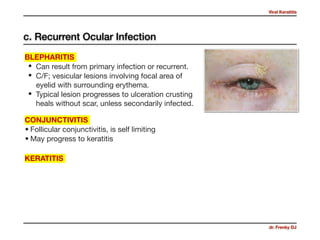
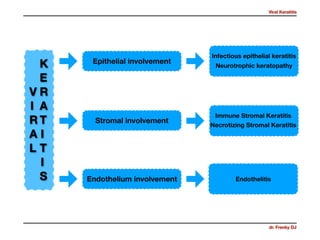
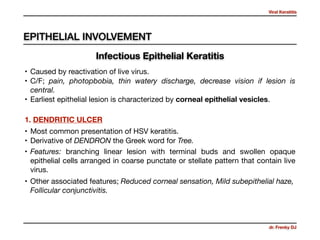
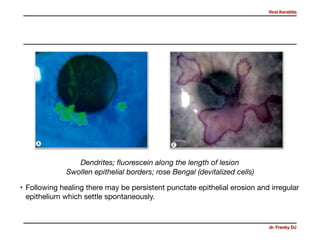
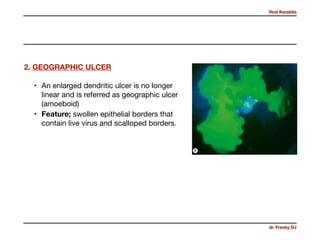
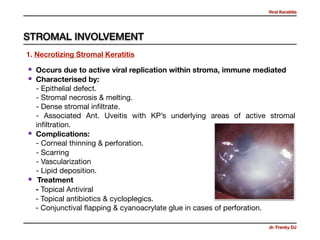
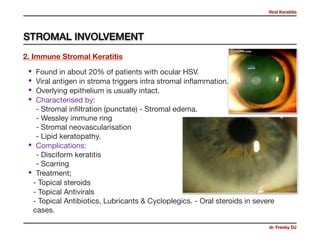
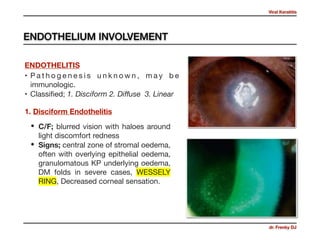

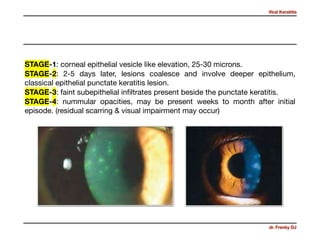

Viral keratitis is commonly caused by herpes simplex virus types 1 and 2 and varicella zoster virus. HSV keratitis typically presents as dendritic ulcers or geographic ulcers on the cornea. It can also cause stromal keratitis. Varicella zoster virus causes herpes zoster infection which presents with a painful rash that follows dermatomal patterns, and can also lead to keratitis. Adenovirus is another common cause and presents as punctate epithelial keratitis that may develop into nummular opacities. Treatment involves topical antivirals and steroids depending on the type and severity of infection.











































































