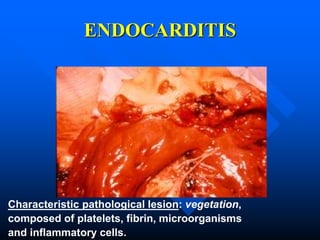
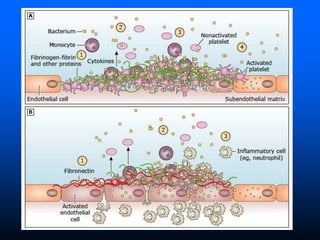
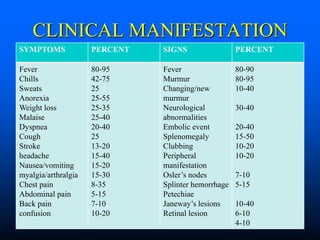
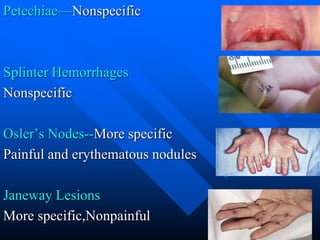
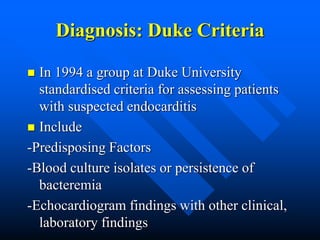
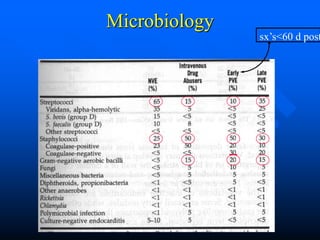
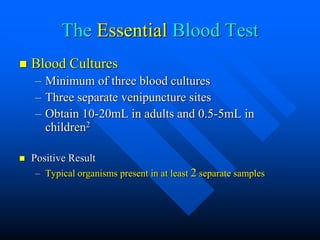
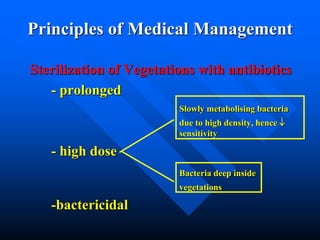
Infective endocarditis is a microbial infection of the heart valves or endocardium. It is characterized by the formation of vegetations composed of platelets, fibrin, microorganisms, and inflammatory cells. It occurs more commonly in males and the elderly. Streptococci and Staphylococcus aureus are the most common causes. Diagnosis involves blood cultures, echocardiography, and applying the Duke criteria. Complications include embolisms, heart failure, and metastatic infections. Treatment involves prolonged antibiotic therapy targeted to the infecting organism. Surgery may be needed for complications or uncontrolled infection. Antibiotic prophylaxis is now restricted to highest risk patients undergoing highest risk procedures.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













