This document provides information on various disorders, pathologies, and diseases that can affect the anterior structures of the eye. It discusses conditions such as:
- Disorders of the eyelashes including trichiasis, distichiasis, and madarosis.
- Benign eyelid lesions including chalazions, molluscum contagiosum, and xanthelasma.
- Malignant eyelid tumors such as basal cell carcinoma, squamous cell carcinoma, and melanoma.
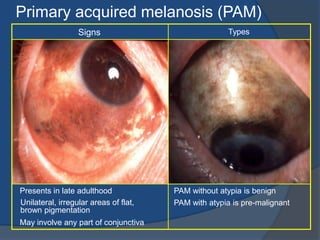
- Conjunctival disorders including bacterial and viral conjunctivitis, vernal conjunctivitis, and pterygium.
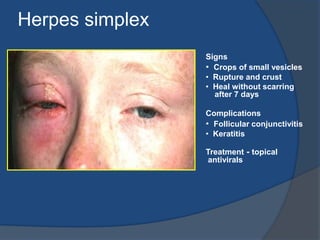
- Corneal pathologies such as infectious keratitis