1. The document discusses diabetic neuropathy, including its classification, clinical characteristics, underlying mechanisms, investigations and pharmacological treatment.
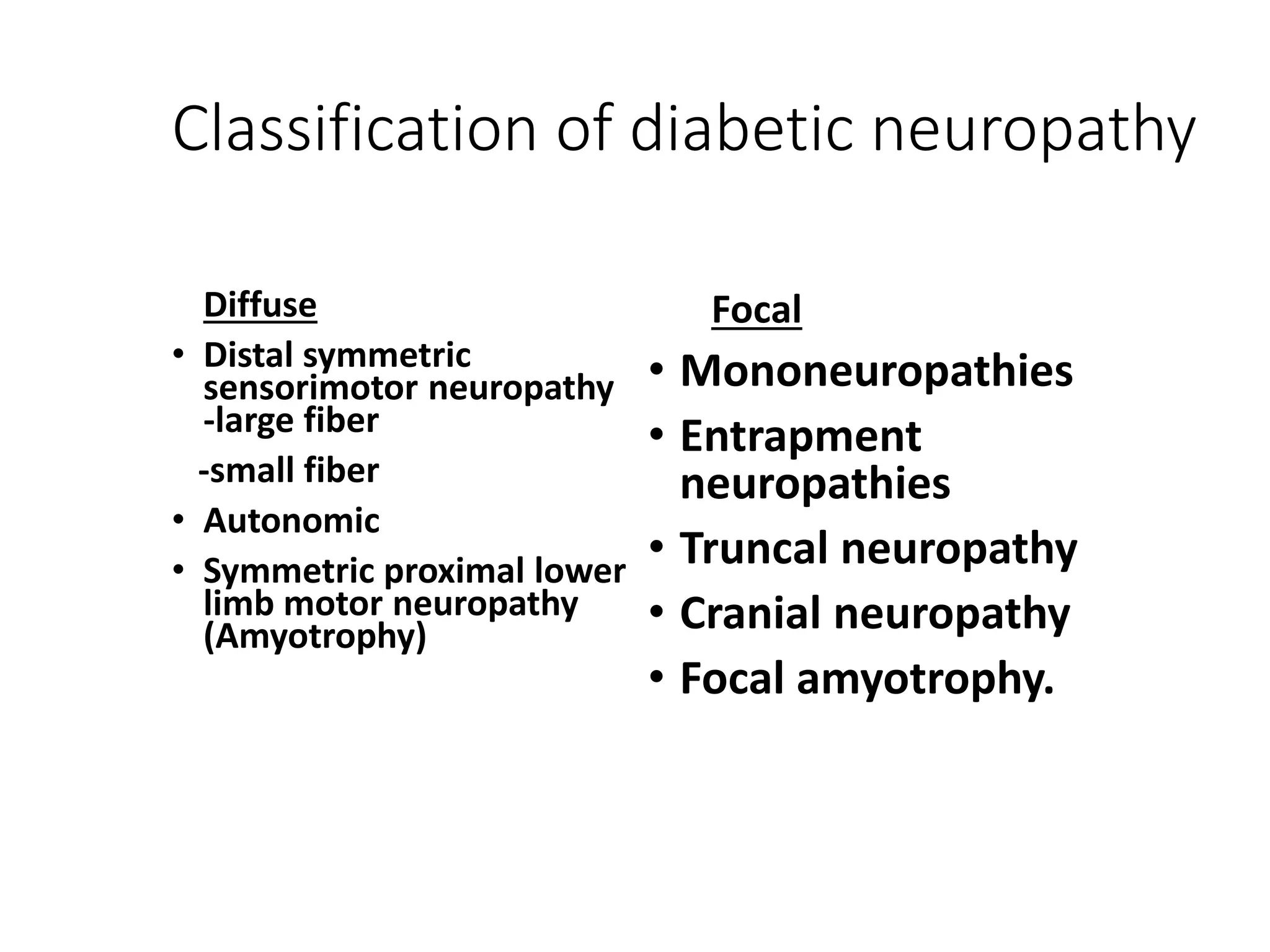
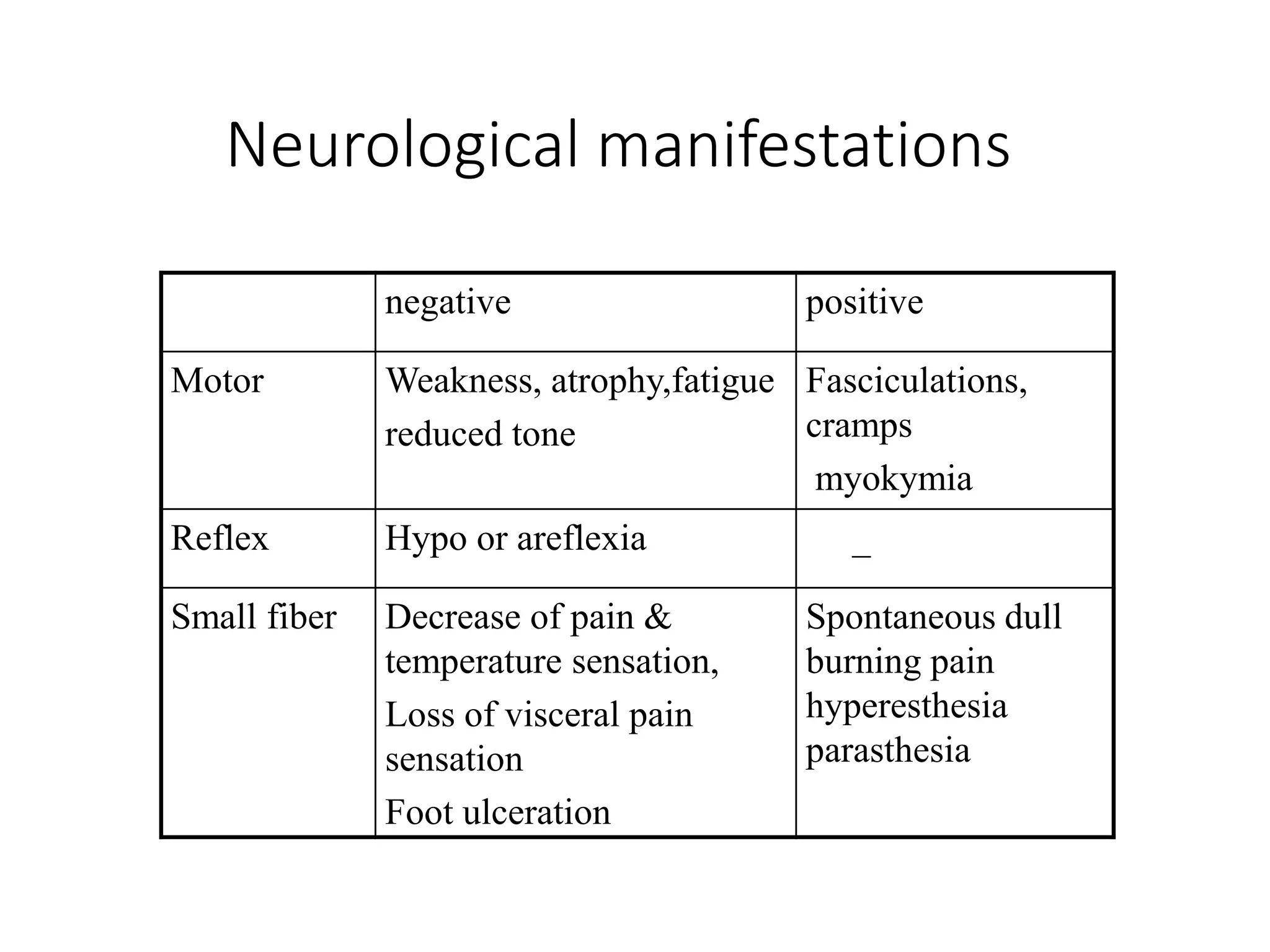
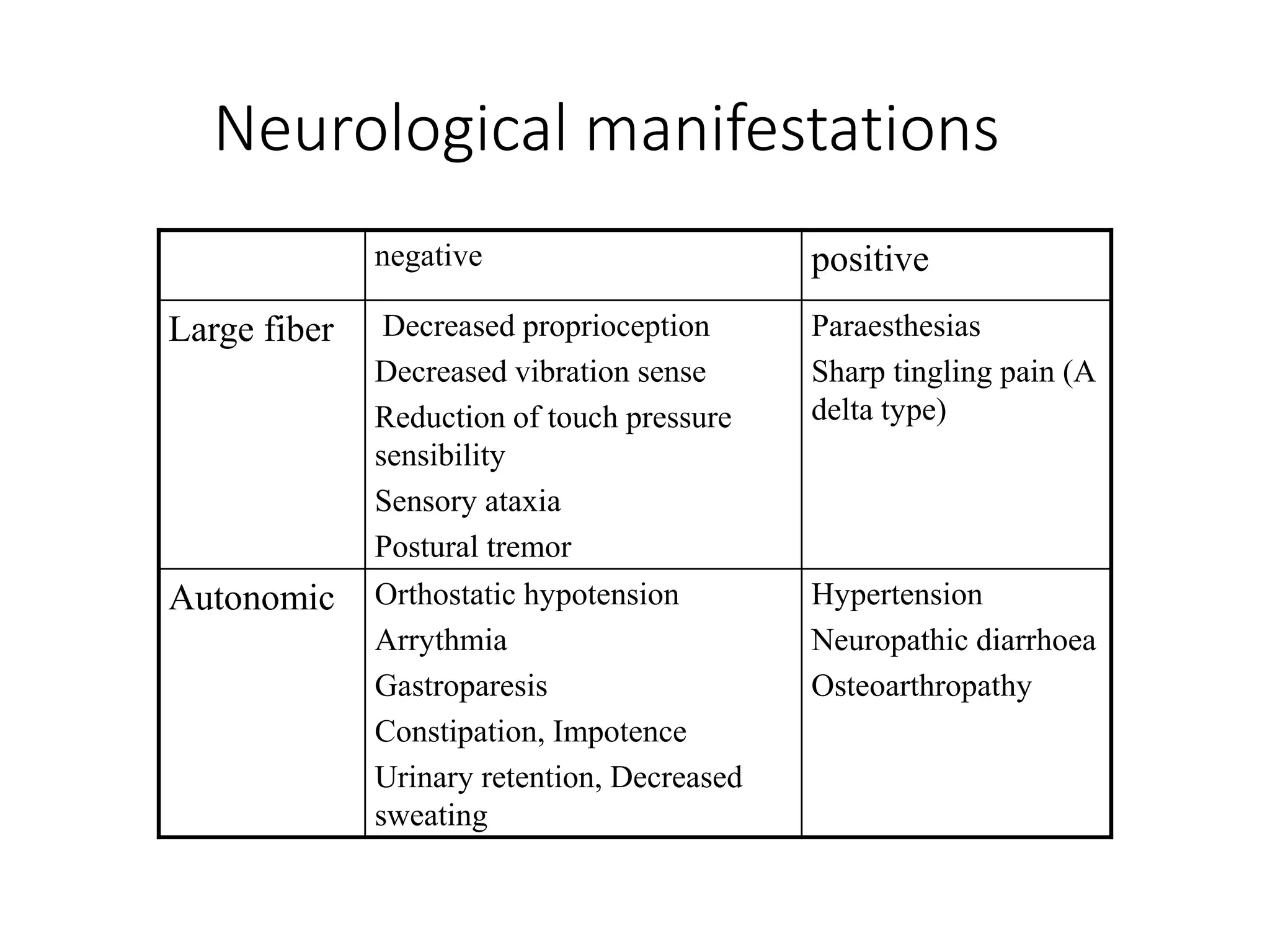
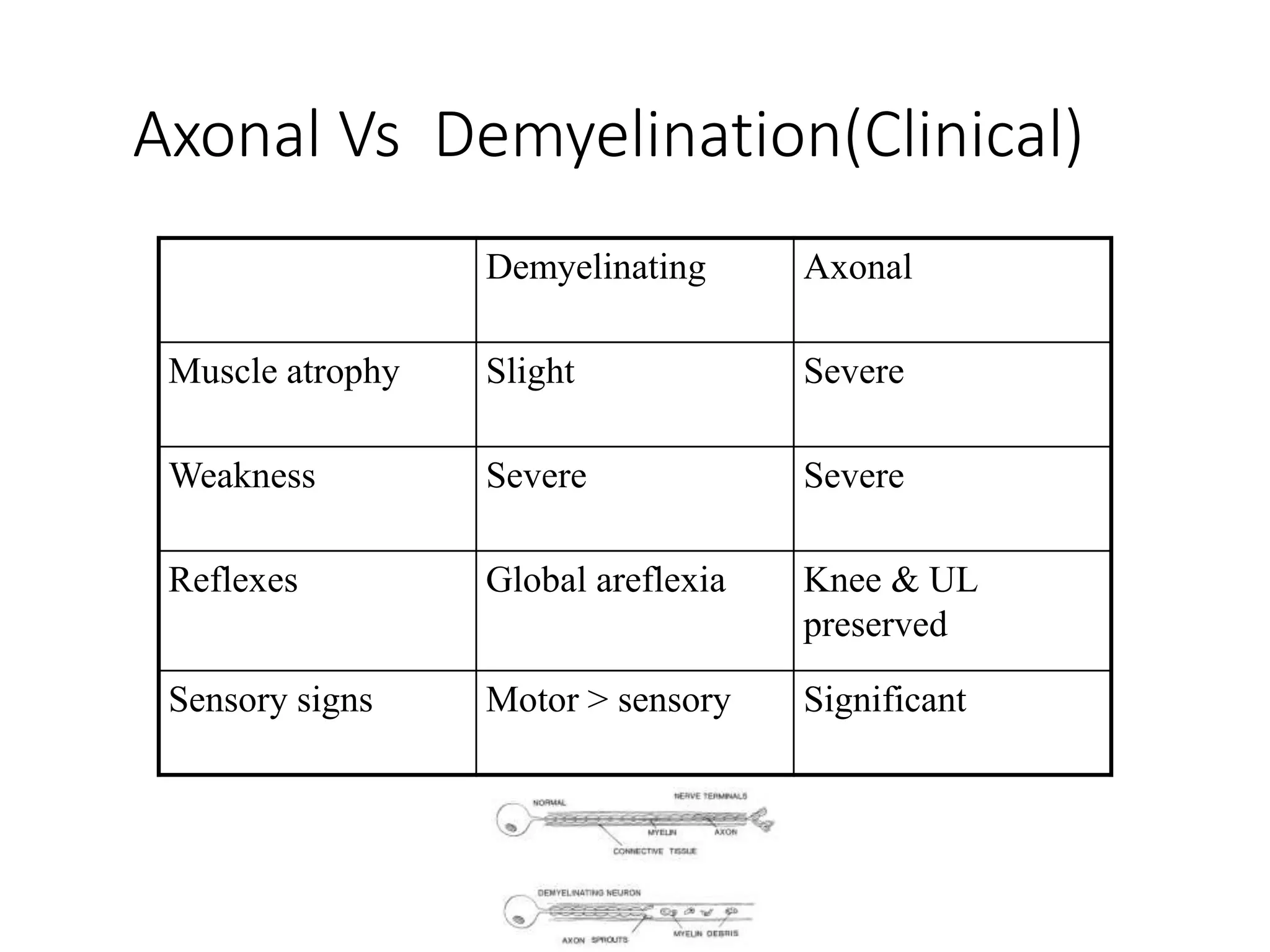
2. Key points include that diabetic neuropathy has many subtypes and involves both large and small nerve fibers. The clinical features progress from negative symptoms like loss of sensation to positive symptoms like pain. Investigations include electrodiagnostic testing and skin or nerve biopsies.
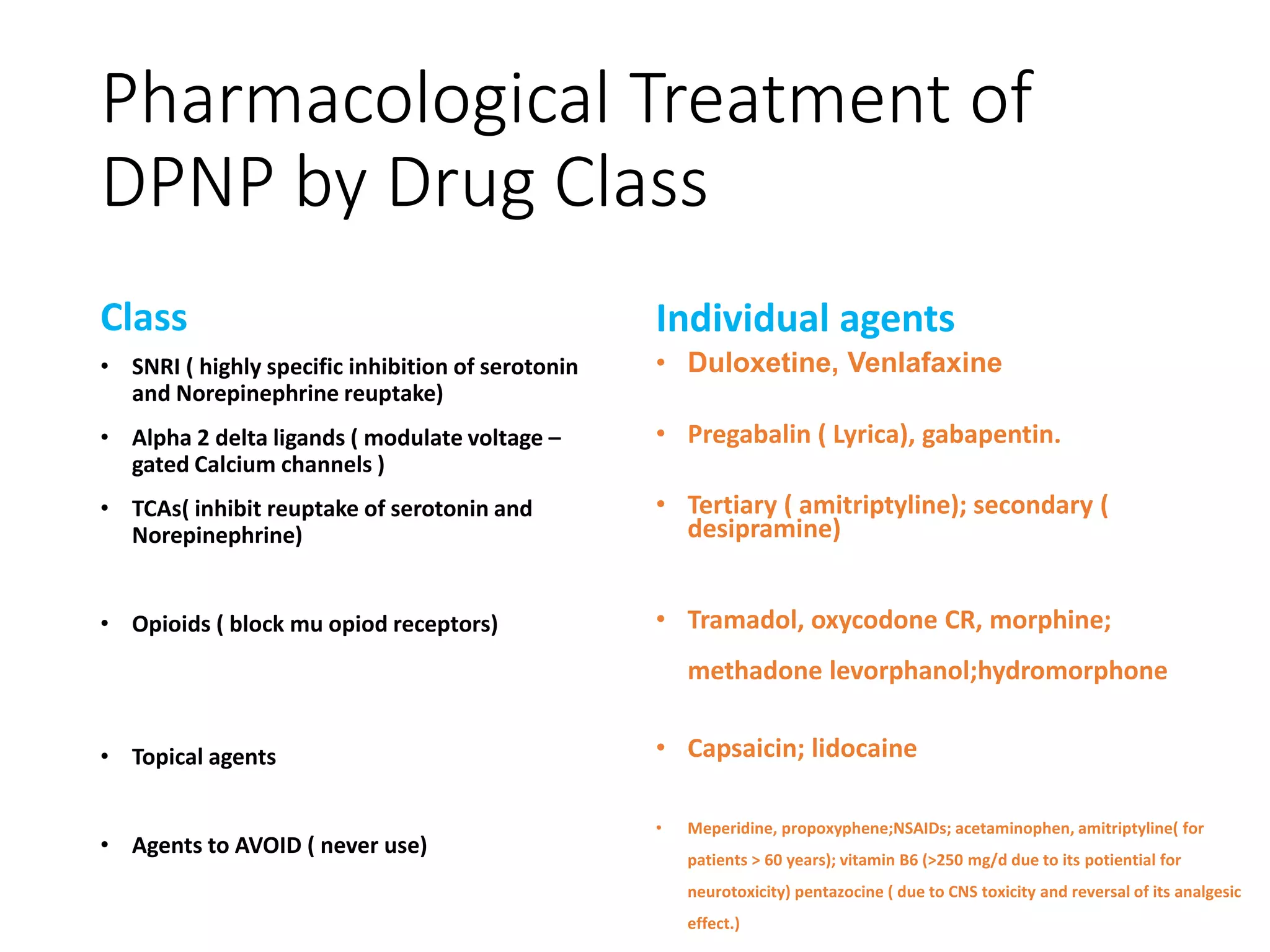
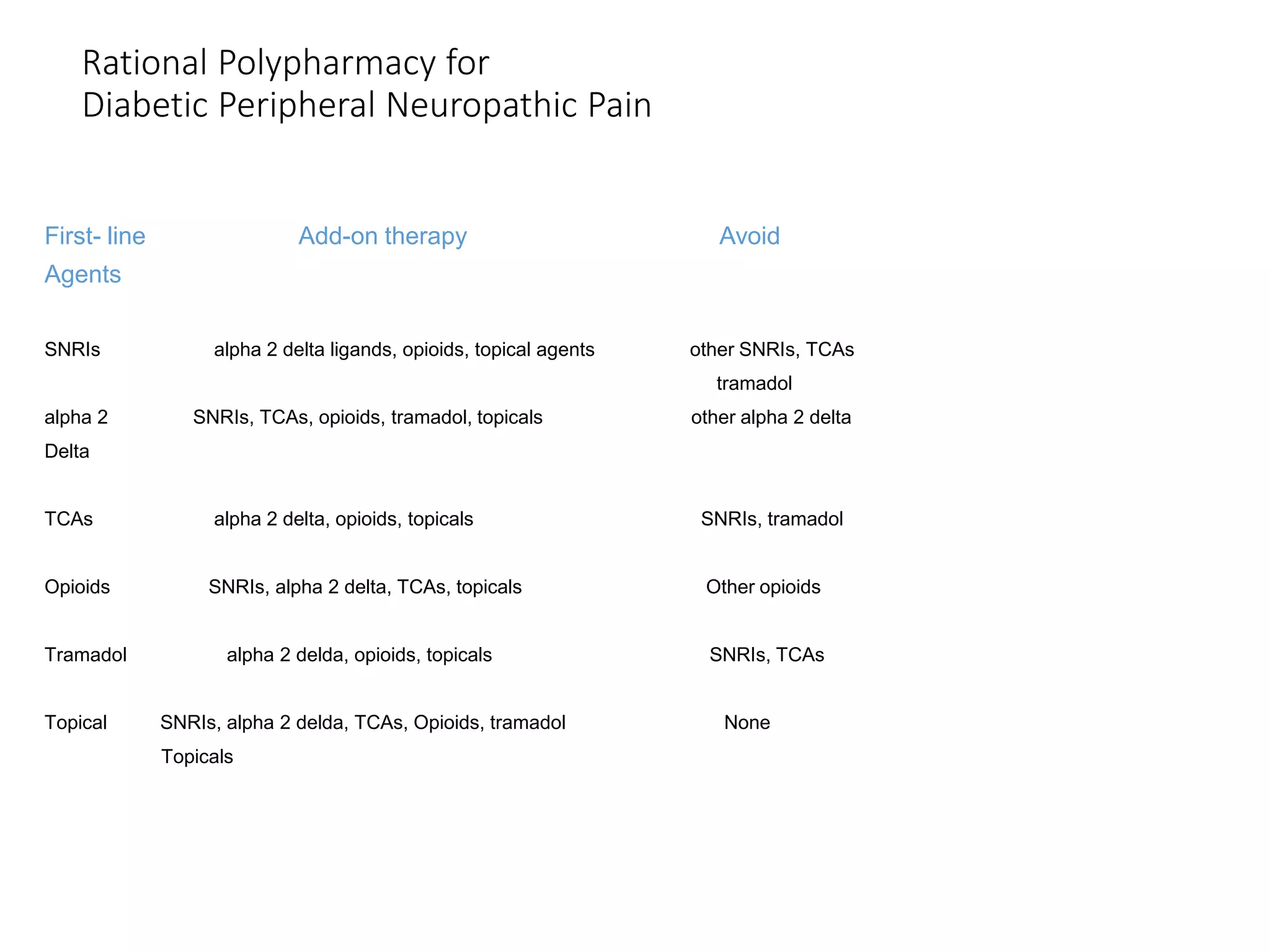
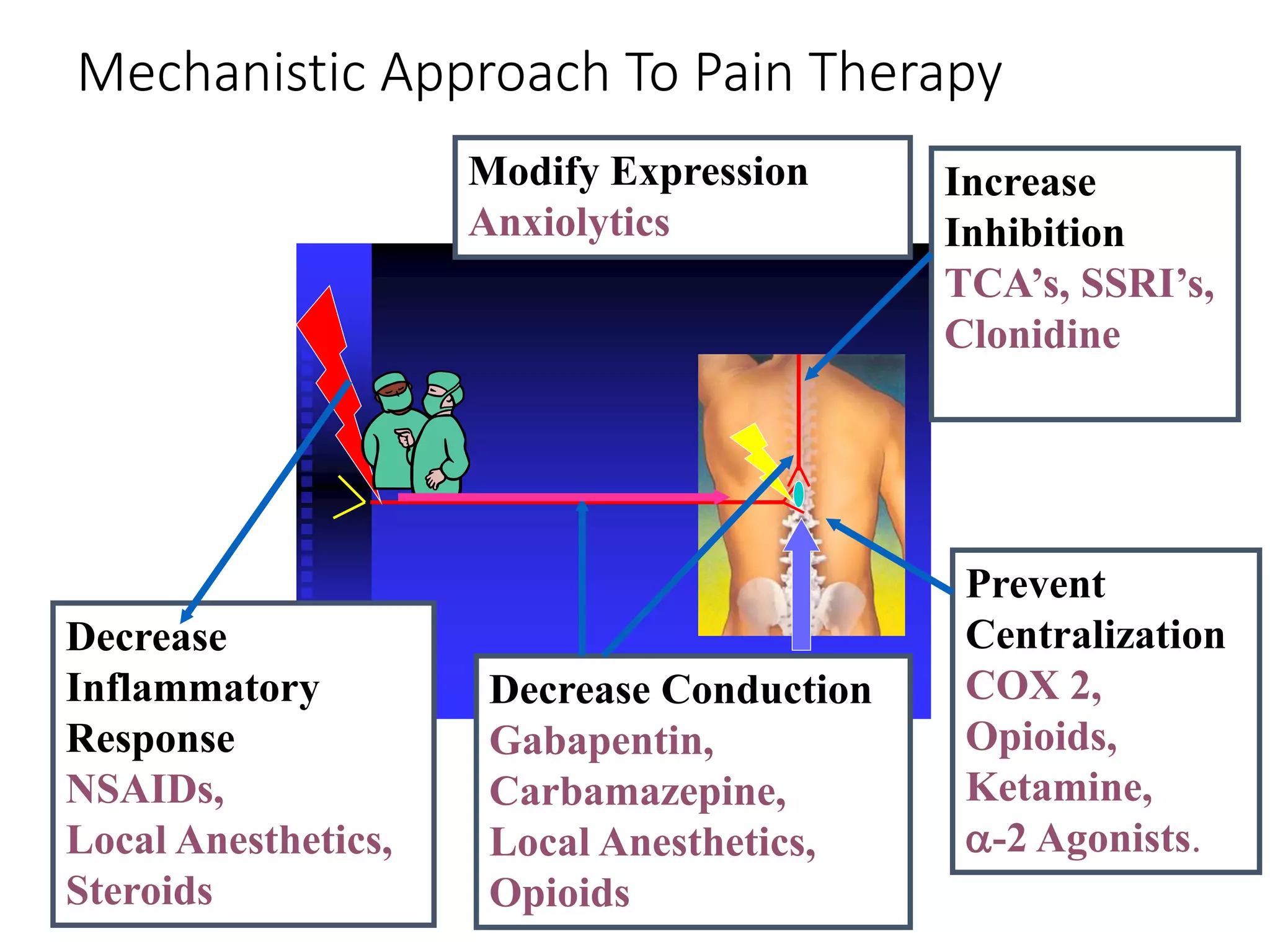
3. Treatment involves first-line options like duloxetine, pregabalin and TCAs. Polypharmacy with combinations from different classes may be considered for refractory cases. Factors like comorbidities, side effects, costs and drug interactions must be evaluated when selecting an individual's treatment plan.