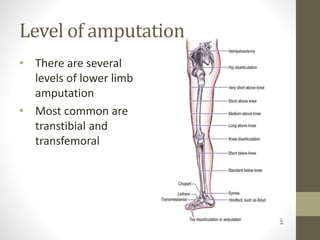
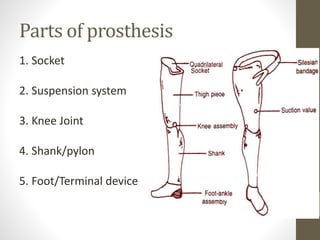
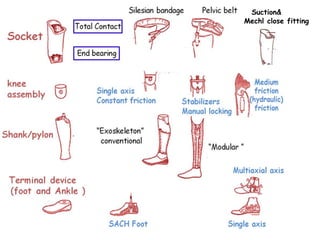
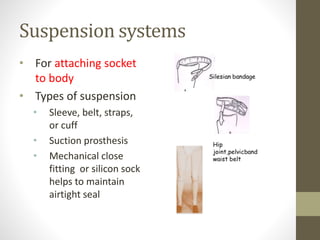
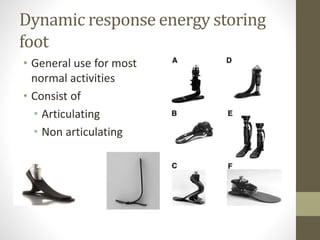
This document provides an overview of lower limb prosthetics. It defines prosthetics as devices that replace missing limbs and discusses their aims of restoring function and mobility. It describes the common levels of lower limb amputation as transtibial and transfemoral. The key components of a lower limb prosthesis are then outlined as the socket, suspension system, knee joint, shank/pylon, and foot/terminal device. Issues related to prosthesis use like skin problems, pain, and ineffective suspension are also summarized.