Downloaded 1,379 times

















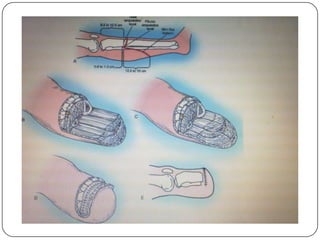












This document provides an outline on below knee (transtibial) amputation. It discusses the relevant anatomy, classification, indications, preoperative preparations, intraoperative procedure, postoperative care/rehabilitation, complications, prosthesis, and situation in the subregion. The goal of amputation is to find an adequate level for healing and prosthetic fitting while addressing the patient's medical conditions through a multidisciplinary approach to rehabilitation.



























































