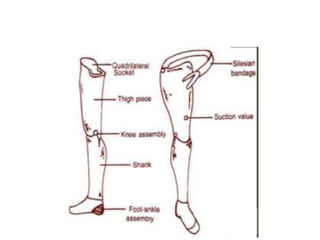
An exoskeletal prosthesis has the strength provided by an outer lamination, while the cosmetic cover is integral. An endoskeletal prosthesis offers more adjustable components but a less durable cosmesis. It consists of lighter materials like aluminum and titanium with interchangeable connectors, knees, and feet, allowing for alignment changes and improved function compared to an exoskeletal prosthesis.