Downloaded 1,255 times
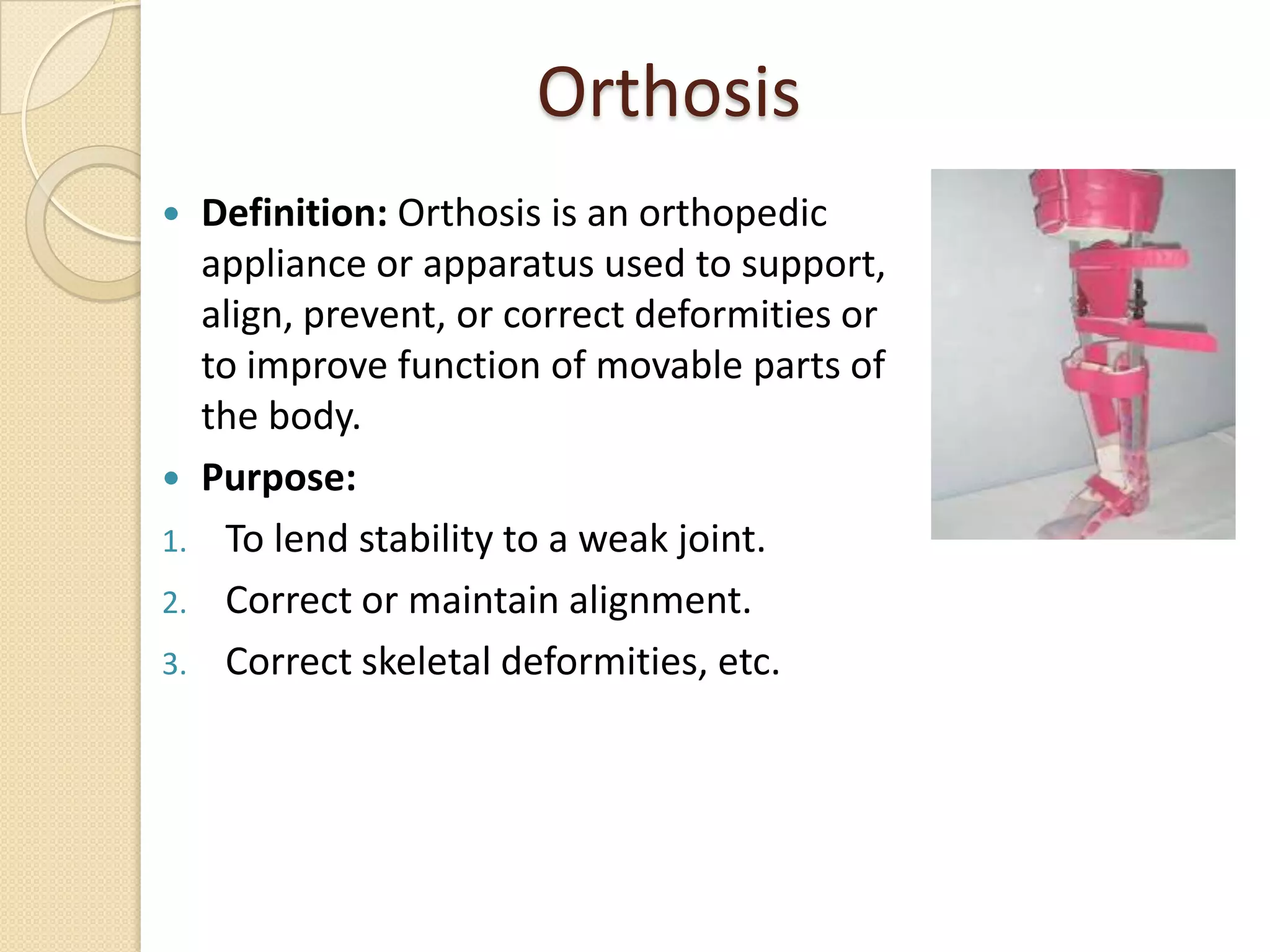
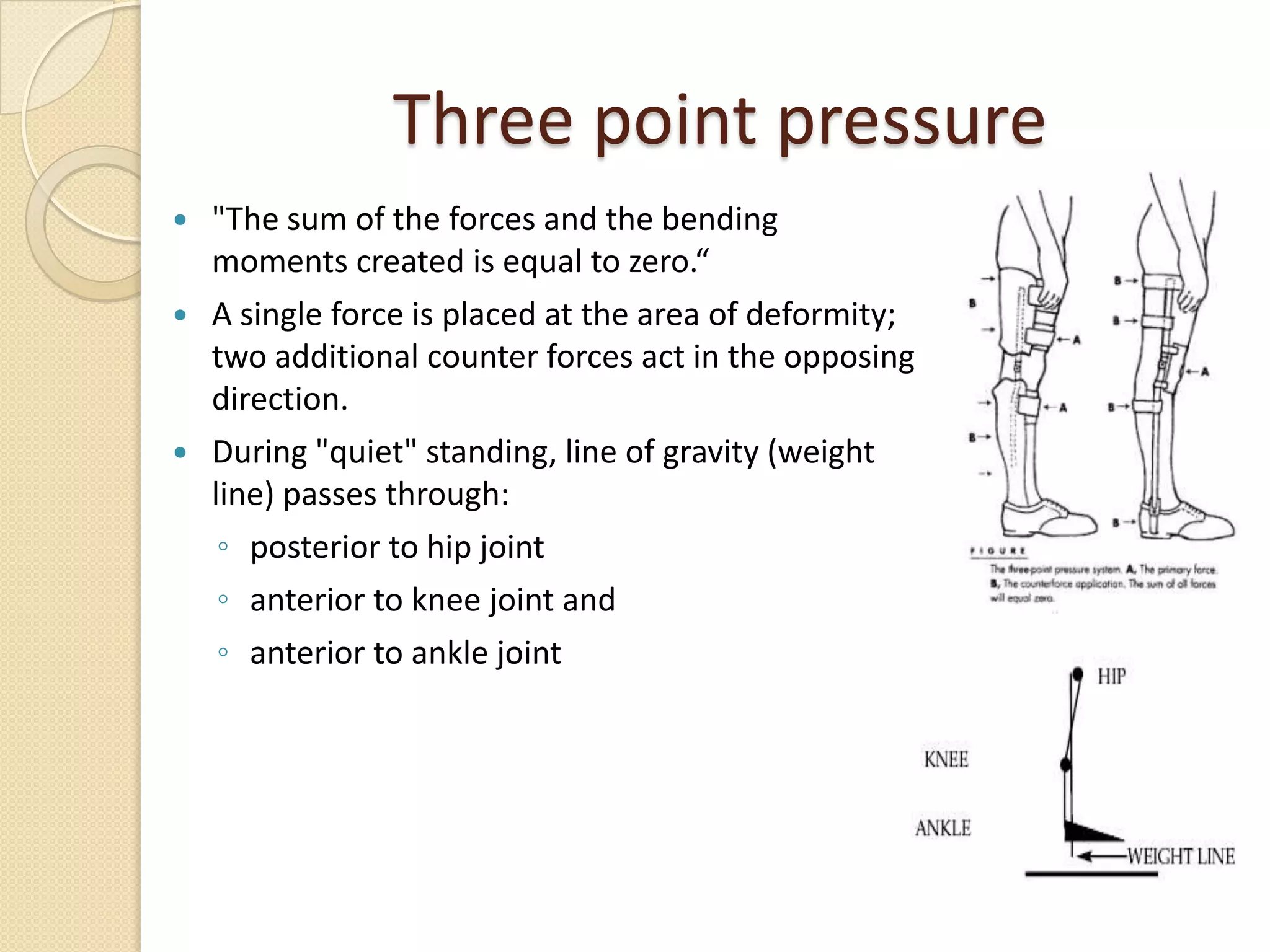




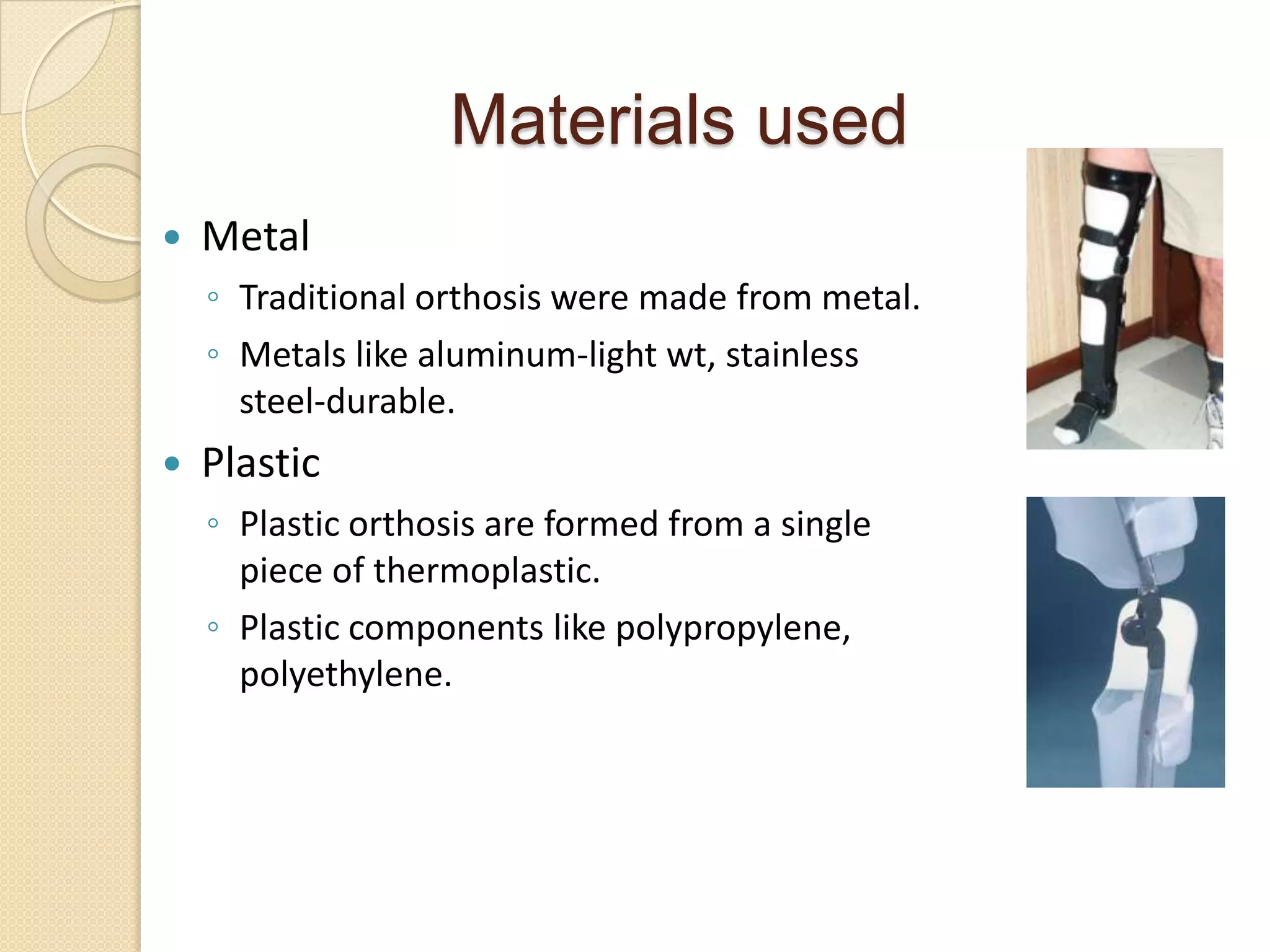
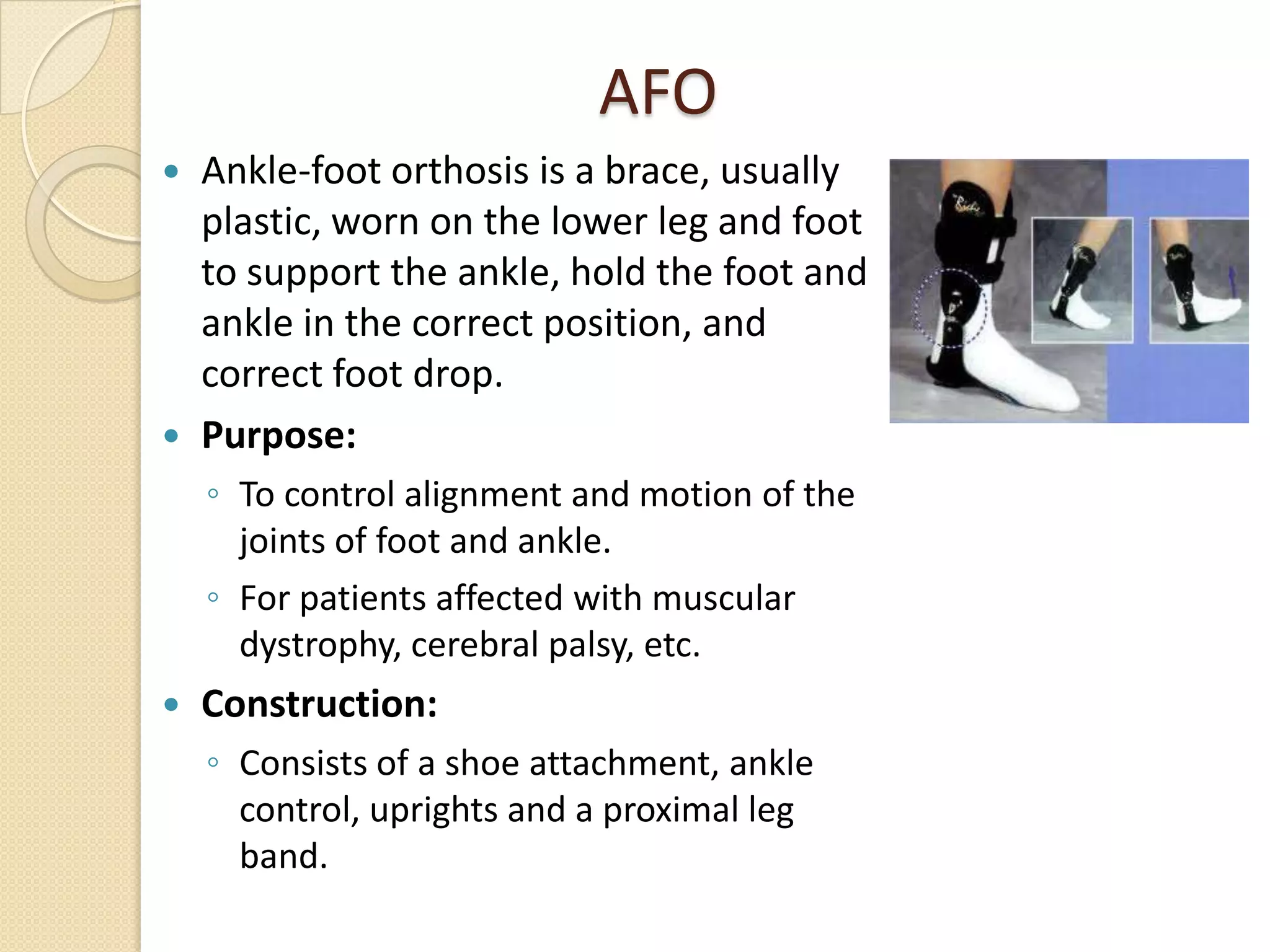
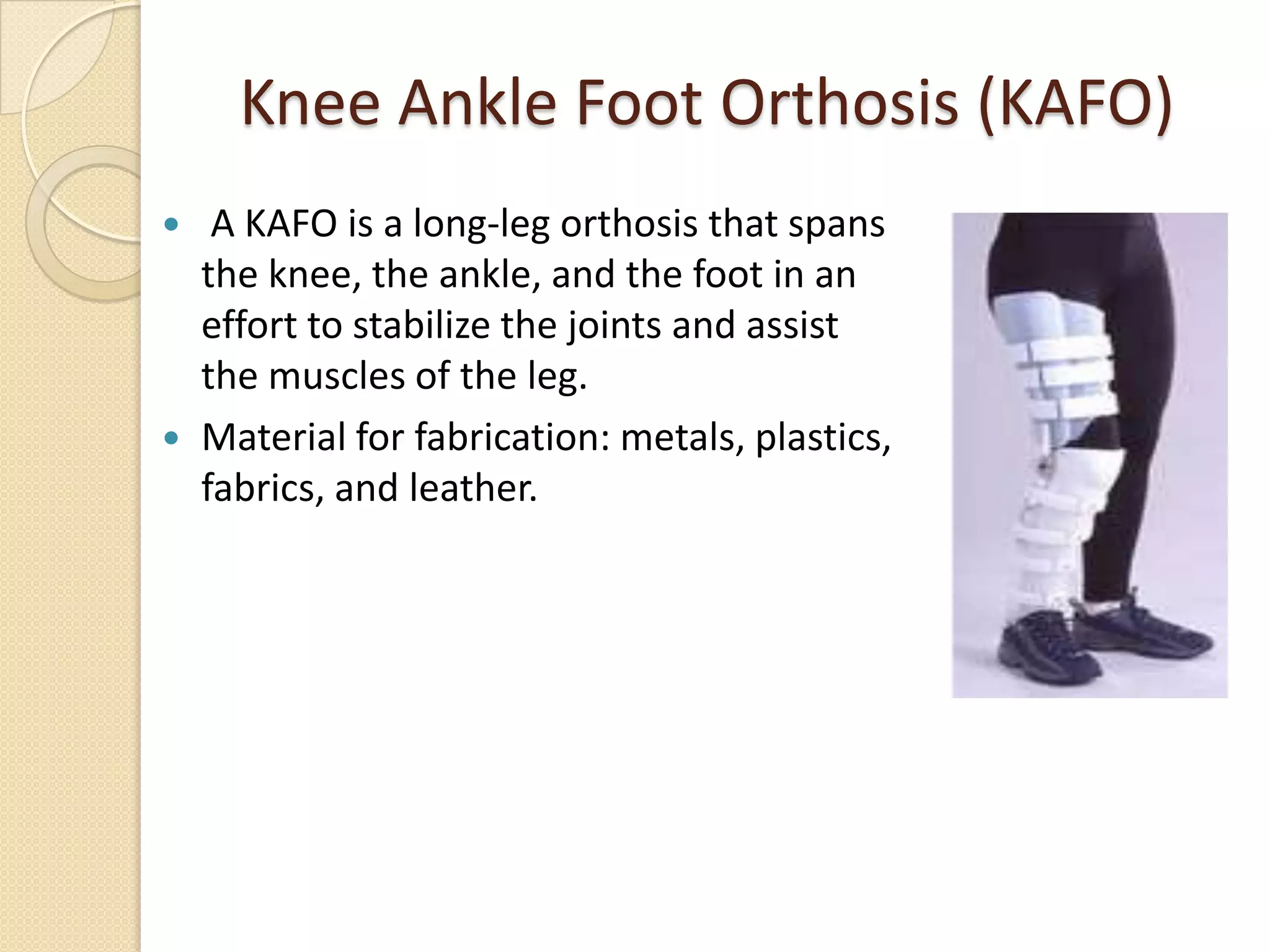


Orthosis are devices used to support weak joints and correct deformities. They work by applying three point pressure and distributing weight across a wide surface area. Common orthosis include ankle foot orthosis (AFO) which support the ankle and foot, knee ankle foot orthosis (KAFO) which stabilize the knee and lower leg, and hip knee ankle foot orthosis (HKAFO) which provide support from the hip to the foot. Orthosis are made of plastic or metal and their design depends on the joints needing support and the individual's condition.

















































































