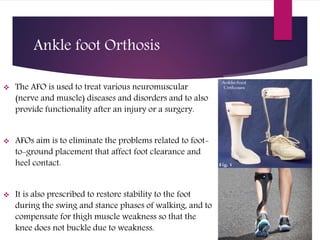
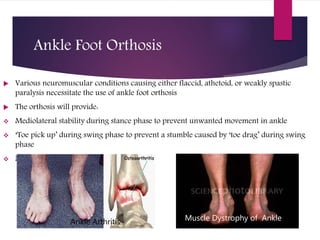
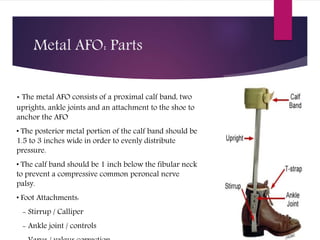
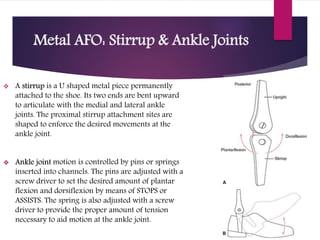
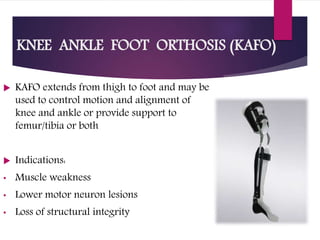
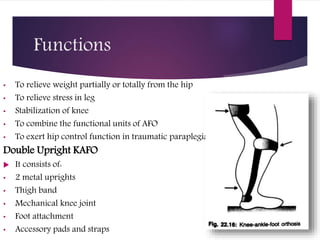
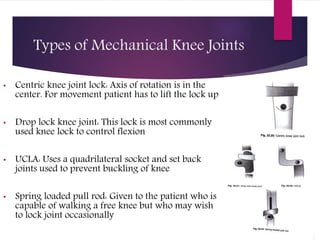
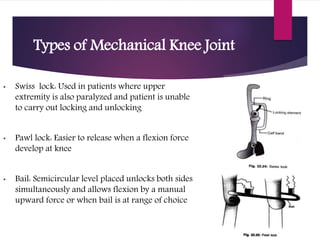
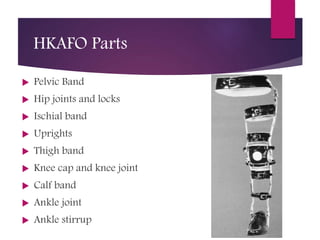
Lower limb orthoses are external devices used to support, stabilize, and correct deformities in the lower limbs, enhancing function and reducing pain. Ankle-foot orthoses (AFOs) address various neuromuscular conditions by improving foot placement during walking and preventing instability, while knee orthoses support joint control for conditions like patellar instability. The document details various types of orthoses including knee-ankle-foot orthoses (KAFOs) and hip orthoses, highlighting their components, indications, and mechanical joint types.