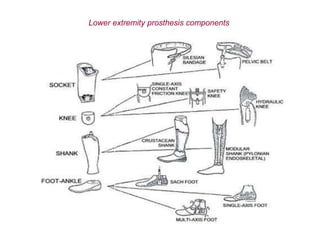
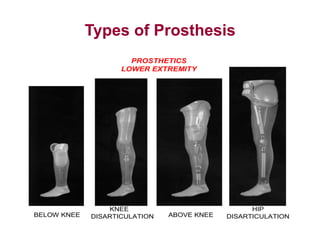
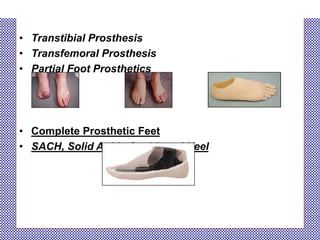
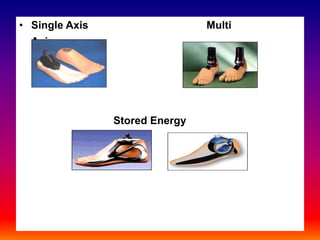
This document discusses lower limb prosthetics. It describes the different levels of lower limb amputation and the basic components of a lower extremity prosthesis, which include the socket, suspension system, knee or articulating joint, shank, and foot or terminal device. It then discusses the different types of feet, shanks, suspensions, sockets, rehabilitation process, role of physical therapy, training, and types of prosthetics for below knee, above knee, and hip disarticulation amputations. Current technology incorporates new materials like carbon fiber to make prosthetics lighter and stronger, as well as use of electronics and myoelectric control.