Downloaded 136 times

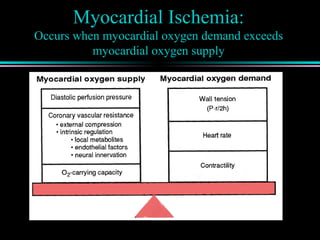
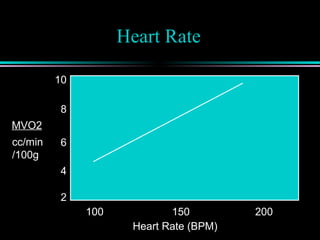
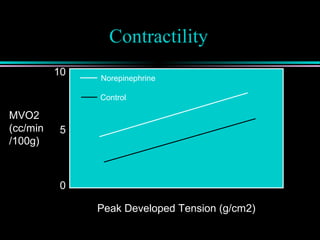
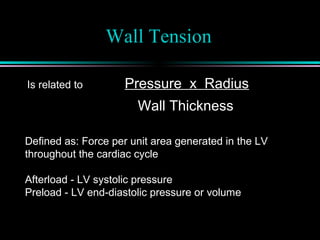
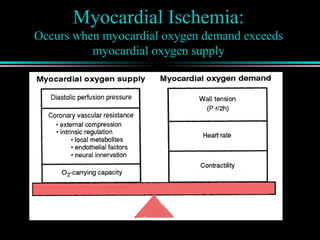
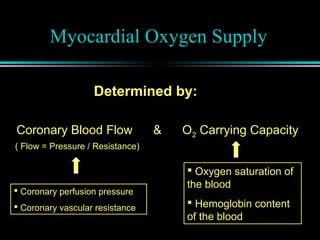
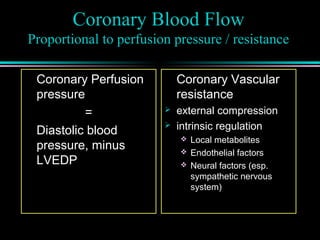
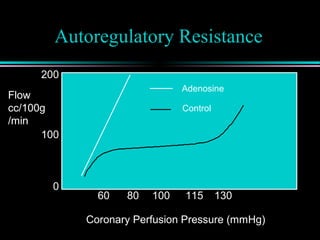
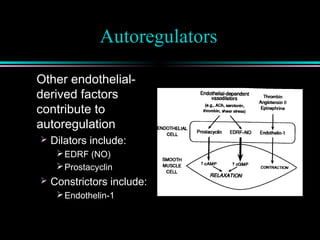
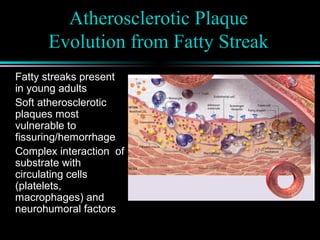
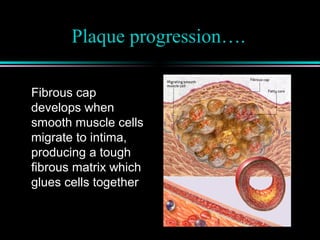
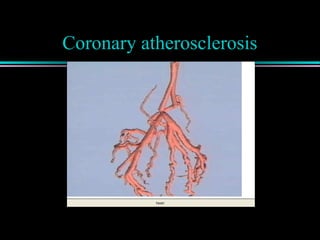
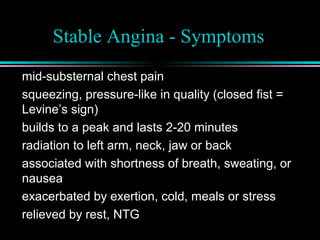
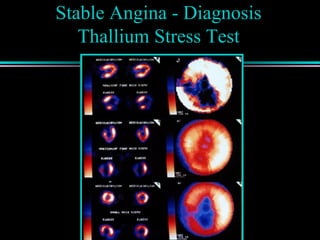
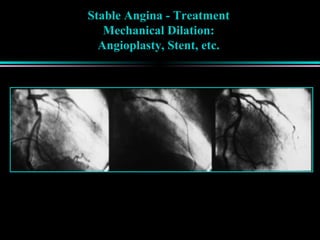
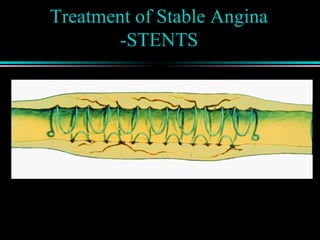
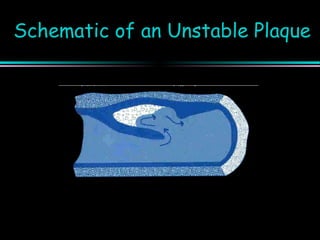
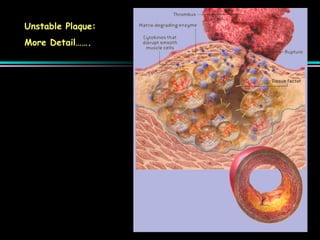
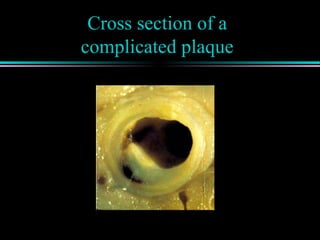
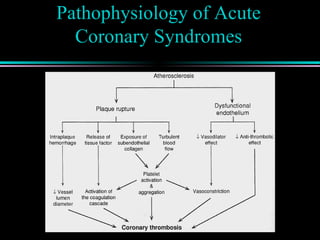
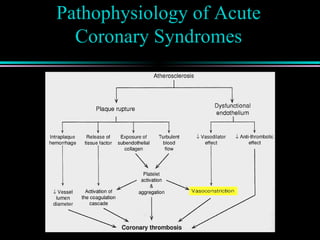
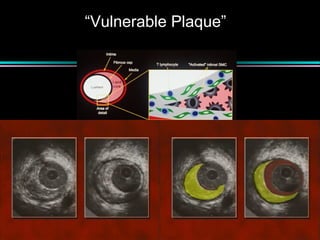
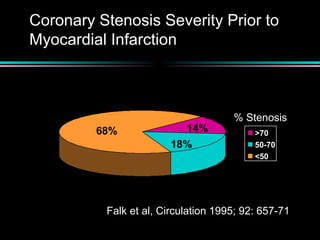
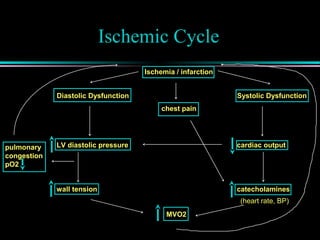
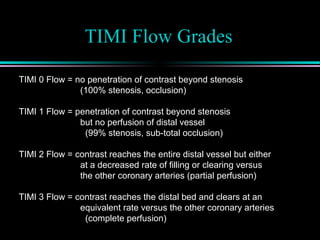
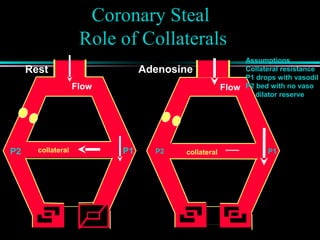
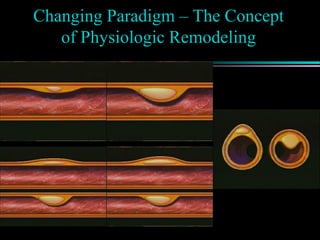

This document discusses the pathophysiology of myocardial ischemia and infarction. It describes how myocardial oxygen demand can exceed supply, leading to ischemia. Factors that determine oxygen demand and supply are explored, including heart rate, contractility, wall tension, coronary blood flow, oxygen carrying capacity of blood, and autoregulatory resistance in arterioles. The progression and vulnerability of atherosclerotic plaque is summarized. Clinical syndromes like stable angina and acute coronary syndromes (unstable angina and myocardial infarction) are defined and their presentations, diagnoses, and treatment approaches are overviewed.











































































































