![ISCHEMIC HEART DISEASES ( IHD )
Resulting from myocardial ischemia [ imbalance
between supply (perfusion), and demand of heart
for oxygenated blood]
In 90% of cases, the cause is reduction in coronary
blood flow due to atherosclerotic coronary arterial
obstruction.
Thus, IHD is often termed coronary artery disease
(CAD) or coronary heart disease (CHD).](https://image.slidesharecdn.com/ischemicheartdiseases-2-130612032217-phpapp02/85/Ischemic-heart-diseases-2-2-320.jpg)
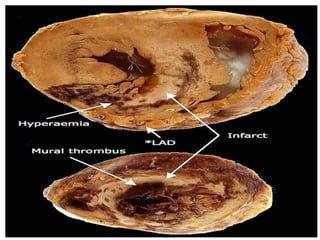
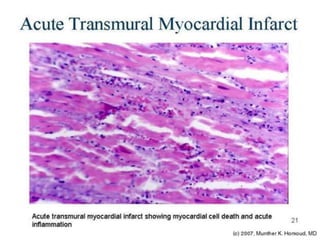

1) Ischemic heart disease results from an imbalance between the heart's demand for oxygenated blood and the supply delivered by the coronary arteries, usually due to atherosclerotic plaque buildup. 2) It manifests as stable angina, unstable angina, myocardial infarction, or sudden cardiac death. 3) Myocardial infarction occurs when a blockage in a coronary artery results in prolonged ischemia and cell death in the heart muscle.





















































![Prac excises 3[1].5](https://cdn.slidesharecdn.com/ss_thumbnails/pracexcises31-150331131154-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















