Downloaded 52 times
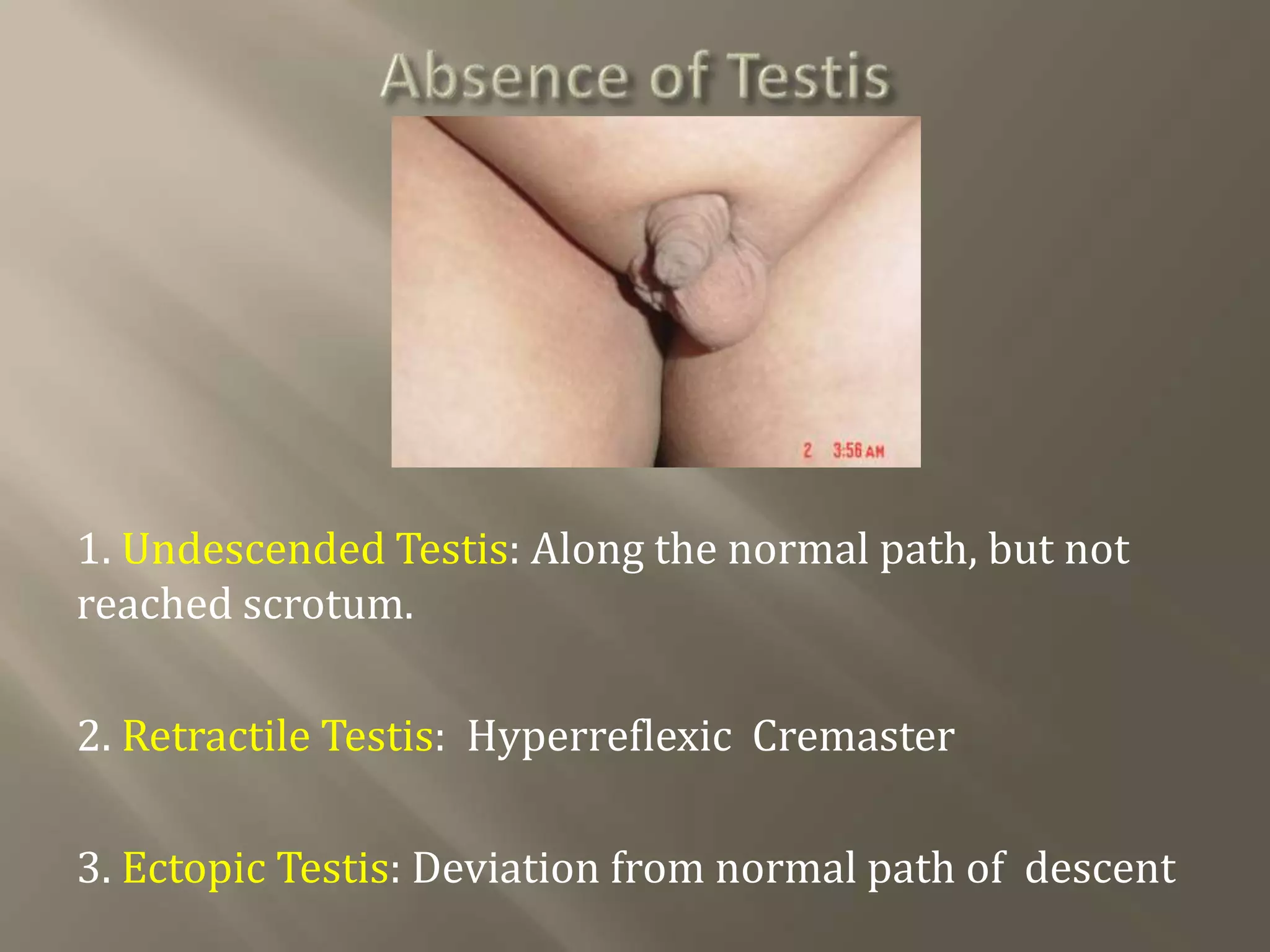

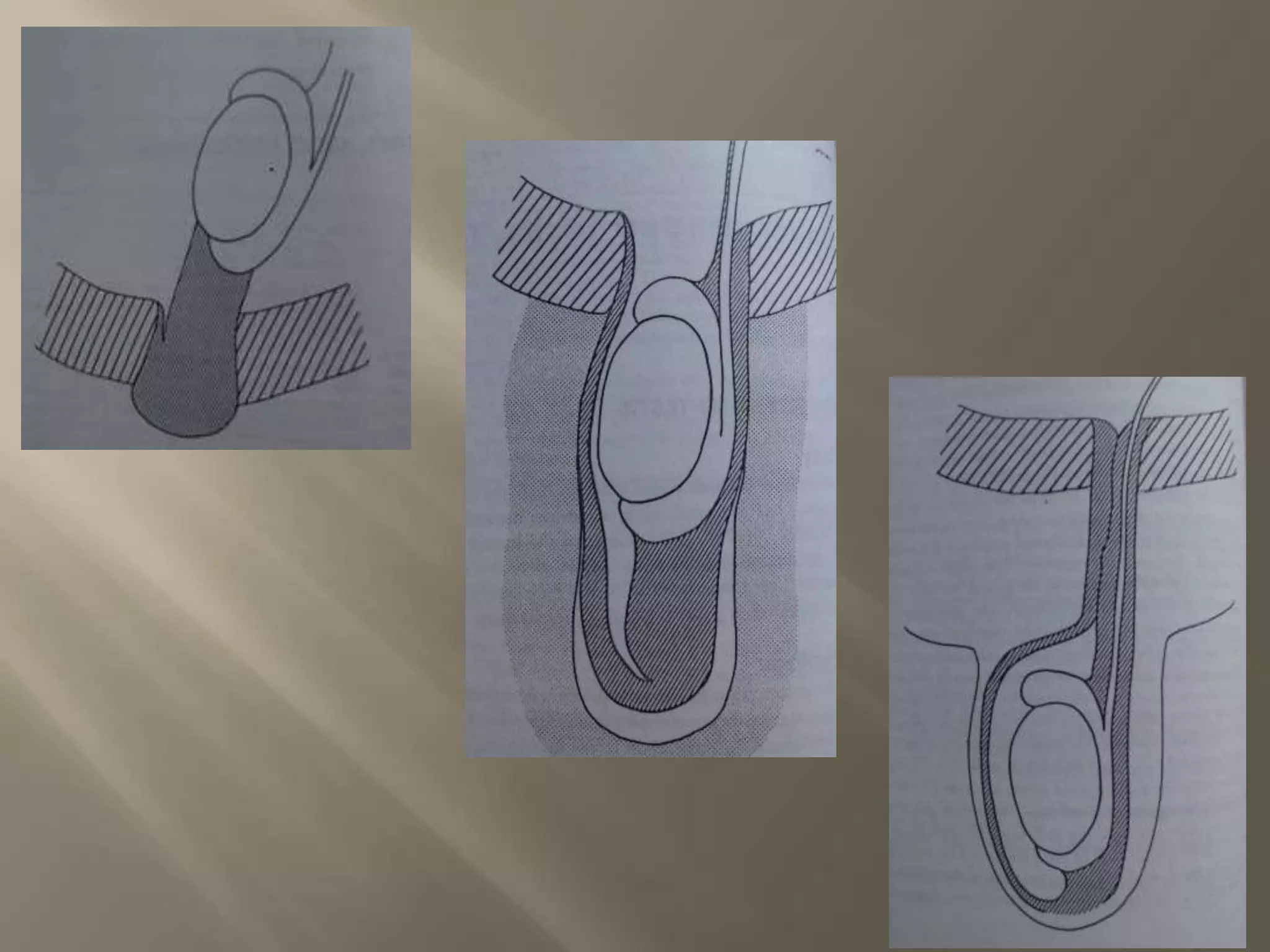
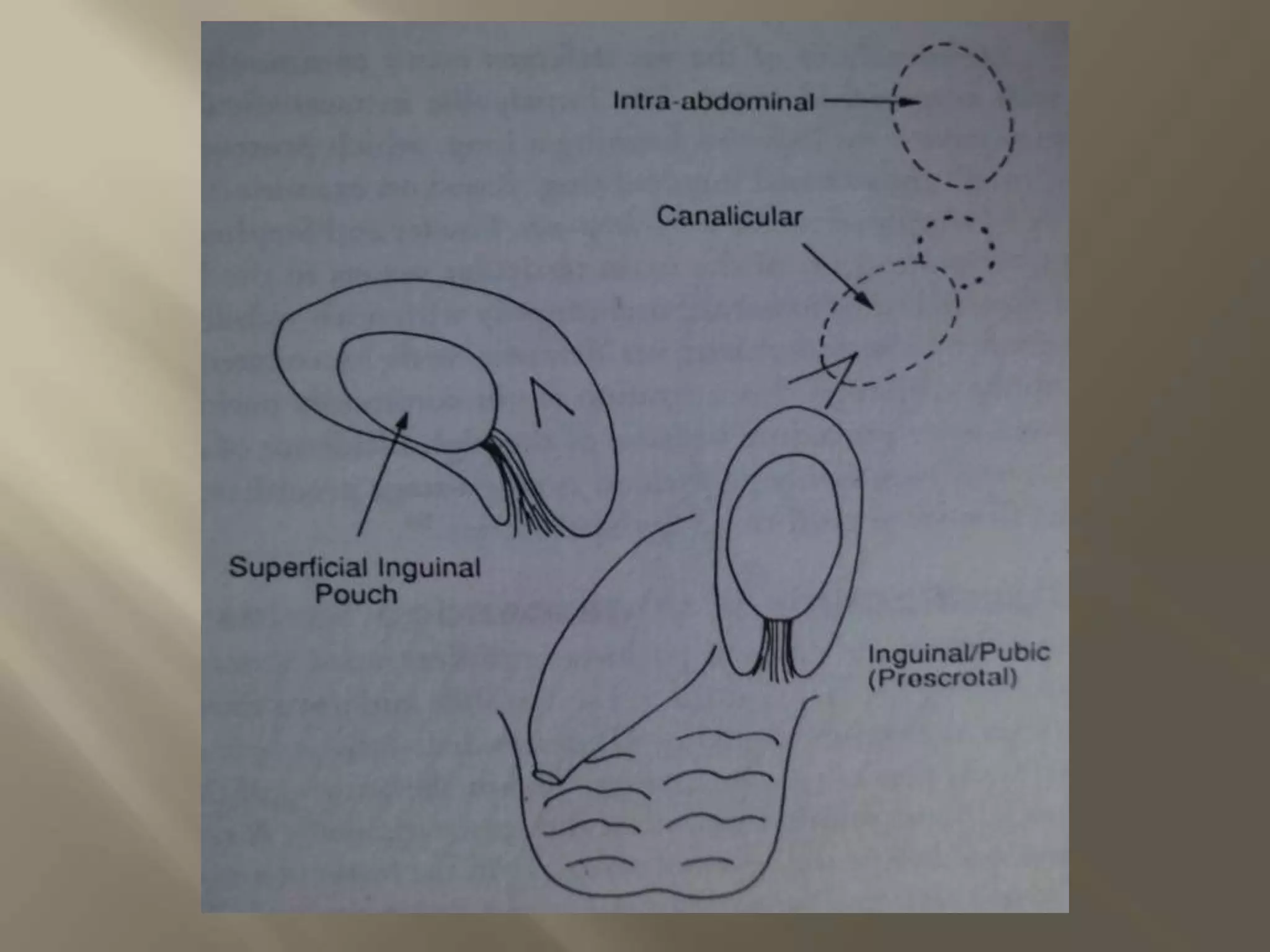

1. Undescended testis occurs when the testis follows the normal path of descent but fails to reach the scrotum. Retractile testis involves a hyperreflexic cremaster muscle. Ectopic testis deviates from the normal path of descent. 2. Testicular descent normally begins at 8 weeks in the abdomen and reaches the scrotum by 9 months. A combination of mechanical and hormonal factors drive descent through the abdominal and inguinal phases. 3. Undescended testis can cause alterations to testicular structure and function, leading to infertility, hernia, torsion and malignancy risks if uncorrected. Orchidopexy is the surgical treatment to


























![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































