Downloaded 1,317 times
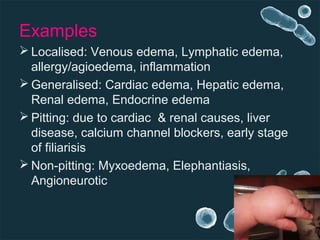
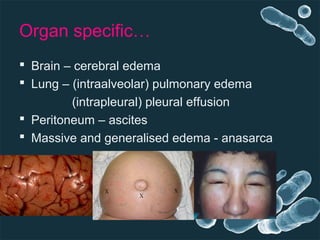
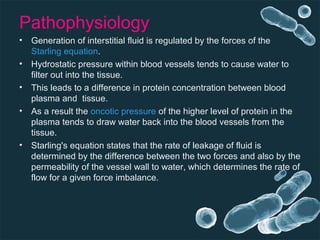
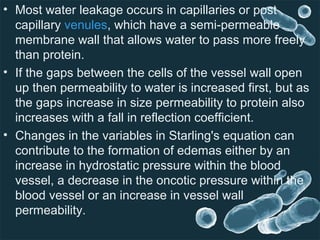



This document discusses the pathophysiology of edema. It defines edema as swelling caused by excess fluid in the interstitial spaces between tissues. Edema can be classified as transudate or exudate based on protein content, and as localized or generalized based on location. The key mechanisms that can cause edema are increased hydrostatic pressure, reduced plasma oncotic pressure, lymphatic obstruction, and sodium and water retention. The movement of fluid between blood vessels and tissues is normally regulated by the balance of hydrostatic and oncotic pressures according to Starling's forces, but imbalances in these forces can result in excess fluid accumulation in the tissues and cause edema.






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
