Downloaded 315 times

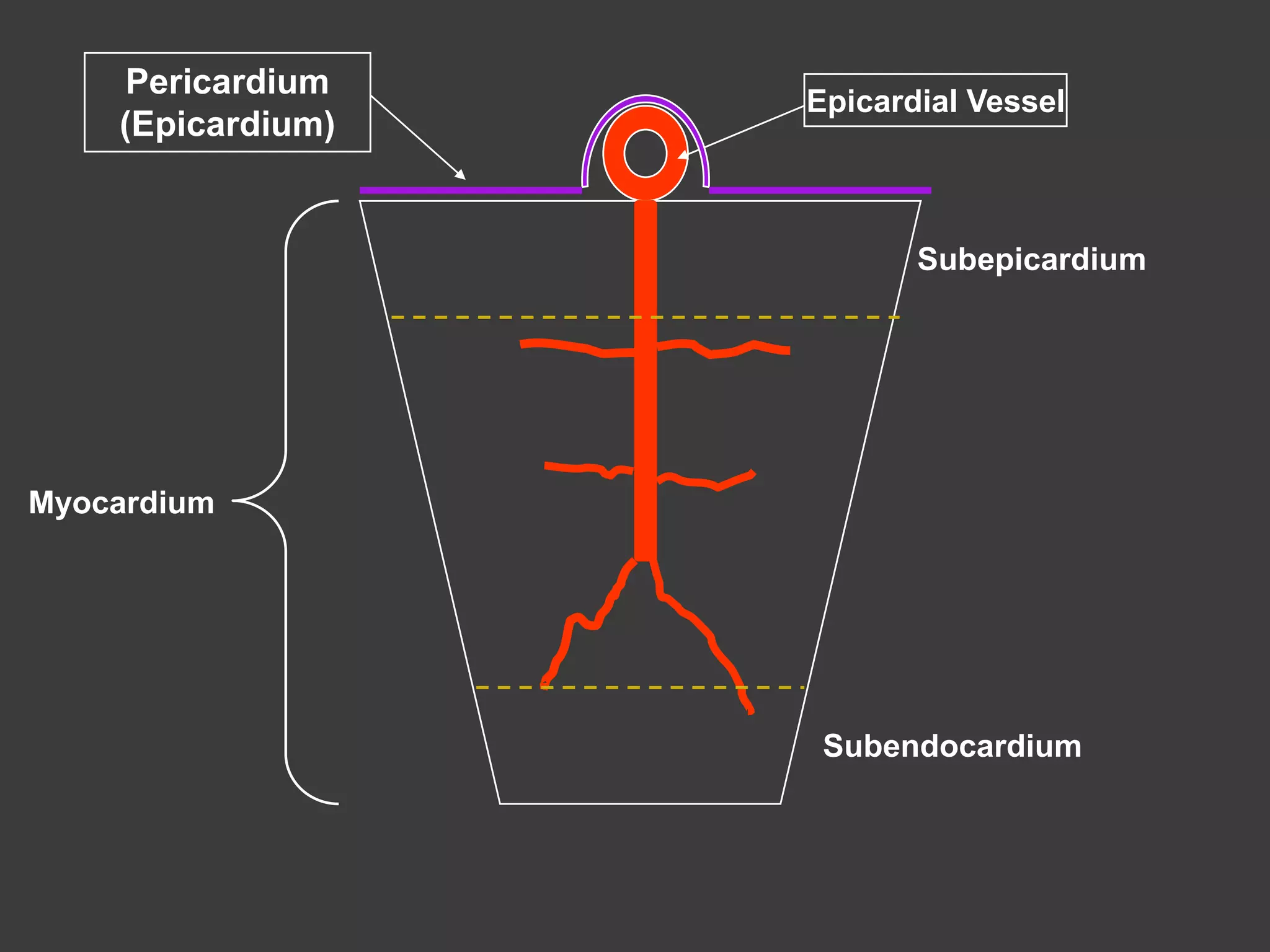








































































The coronary circulation supplies blood to the heart muscle. The right and left coronary arteries branch to form a dense capillary network around each cardiac muscle cell. Coronary blood flow is regulated by metabolic demand of the heart as well as mechanical factors related to the cardiac cycle. During systole, compressive forces within the heart reduce coronary flow, while flow increases during diastole when the vessels dilate. Multiple chemical and neural factors also control resistance within the coronary vasculature to match blood supply with myocardial oxygen requirements. Imbalances can lead to ischemia if demand outpaces supply.











































































