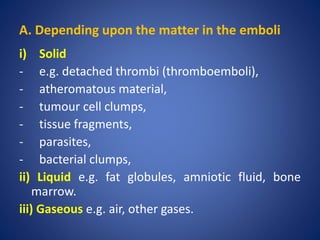
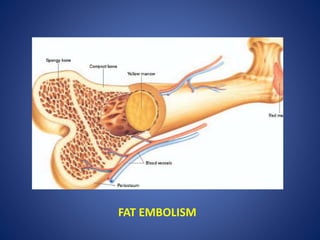
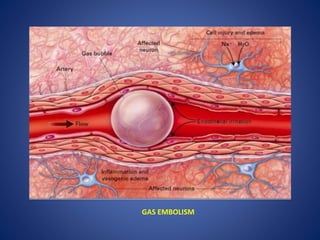
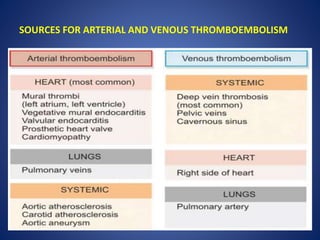
This document defines and describes different types of embolism. The most common type is thromboembolism, which occurs when a thrombus or part of a thrombus breaks off and is carried by the bloodstream. Pulmonary thromboembolism is a significant type that occurs when thrombi travel to the lungs and obstruct the pulmonary arteries. Other types include fat, air, gas and paradoxical embolisms. Air embolism can be venous, entering systemic veins during surgery or trauma, or arterial, entering the lungs during procedures like angiography. Decompression sickness is a form of gas embolism that affects divers or those exposed to changes in atmospheric pressure.