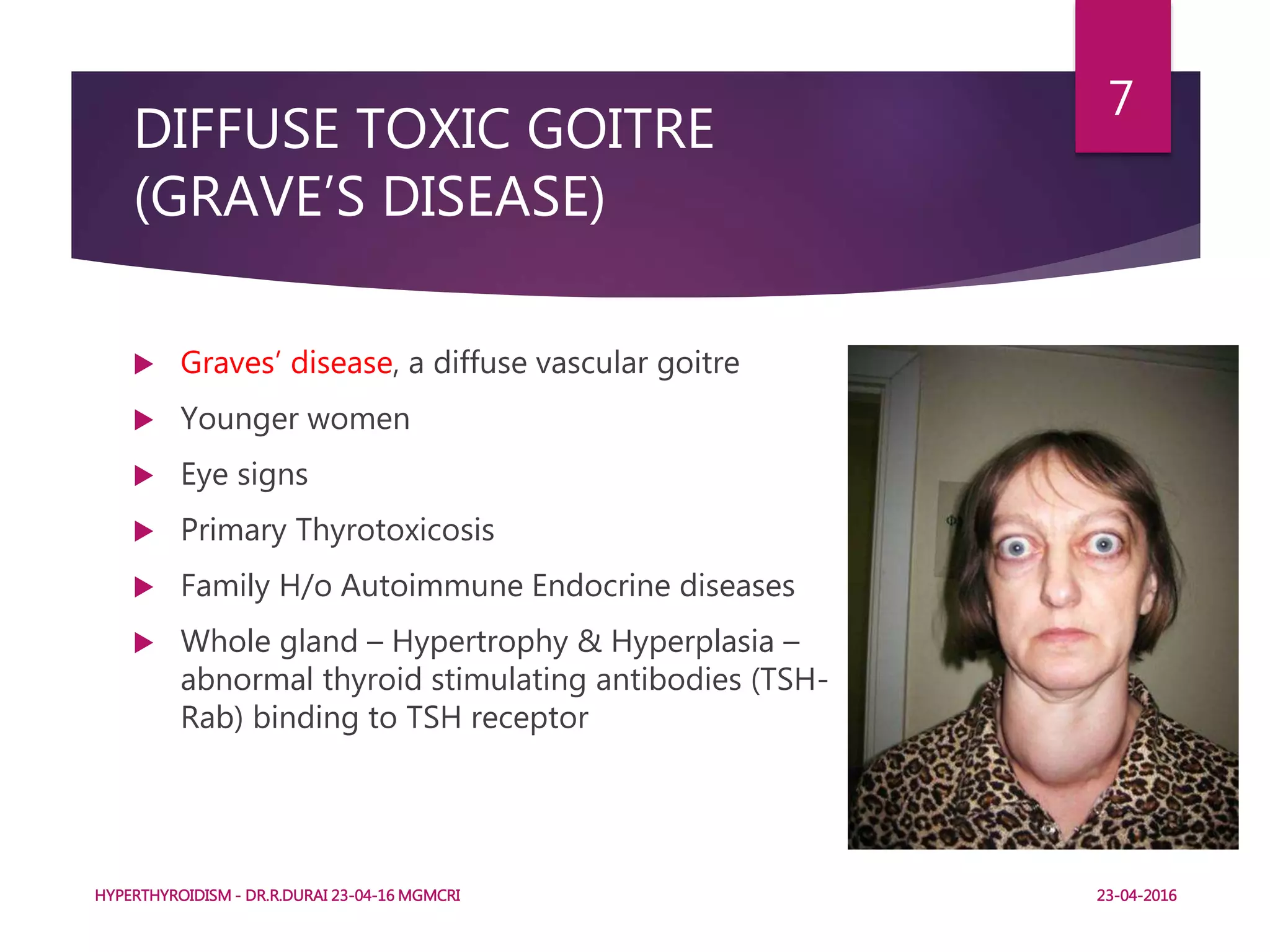
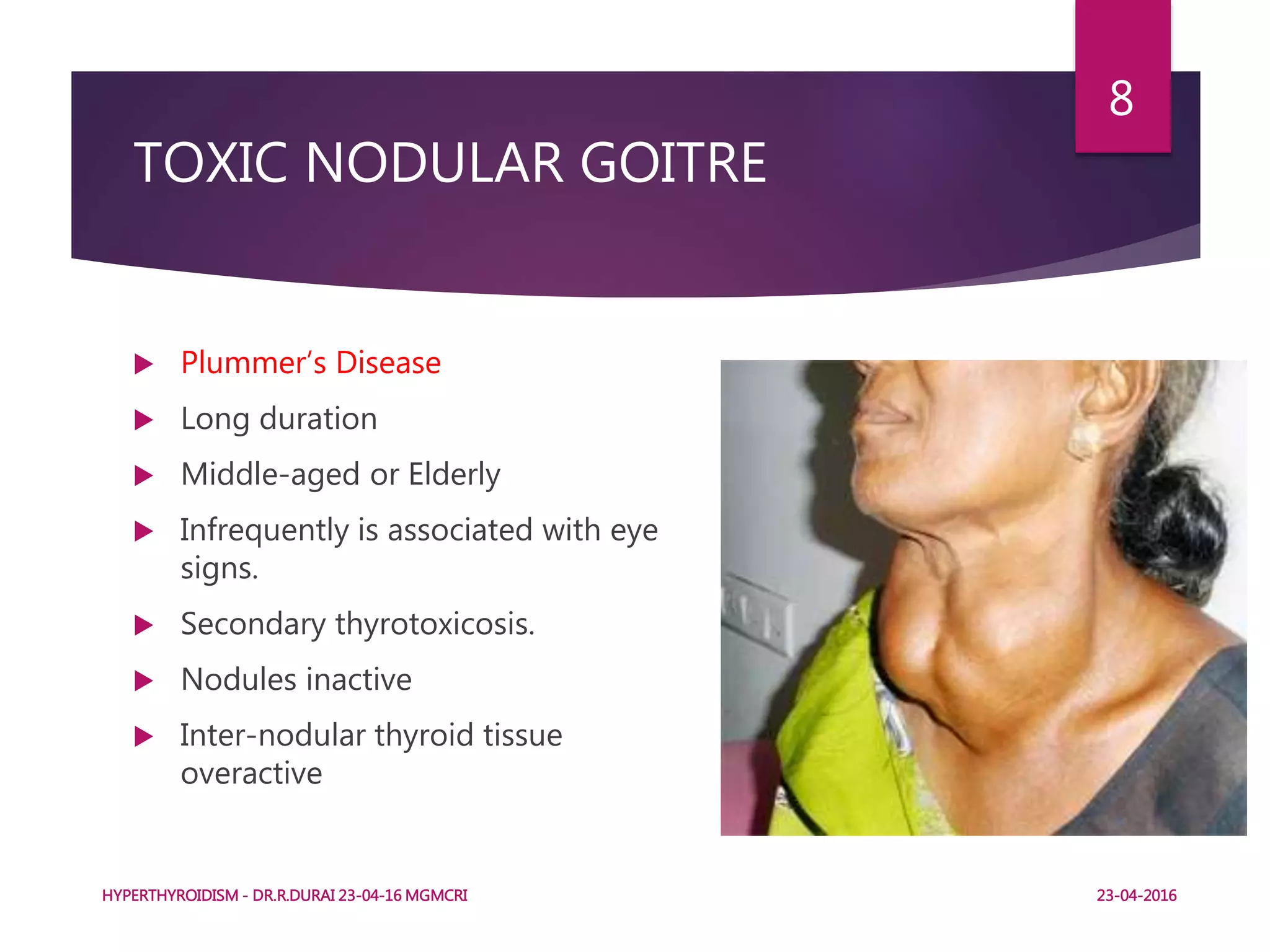
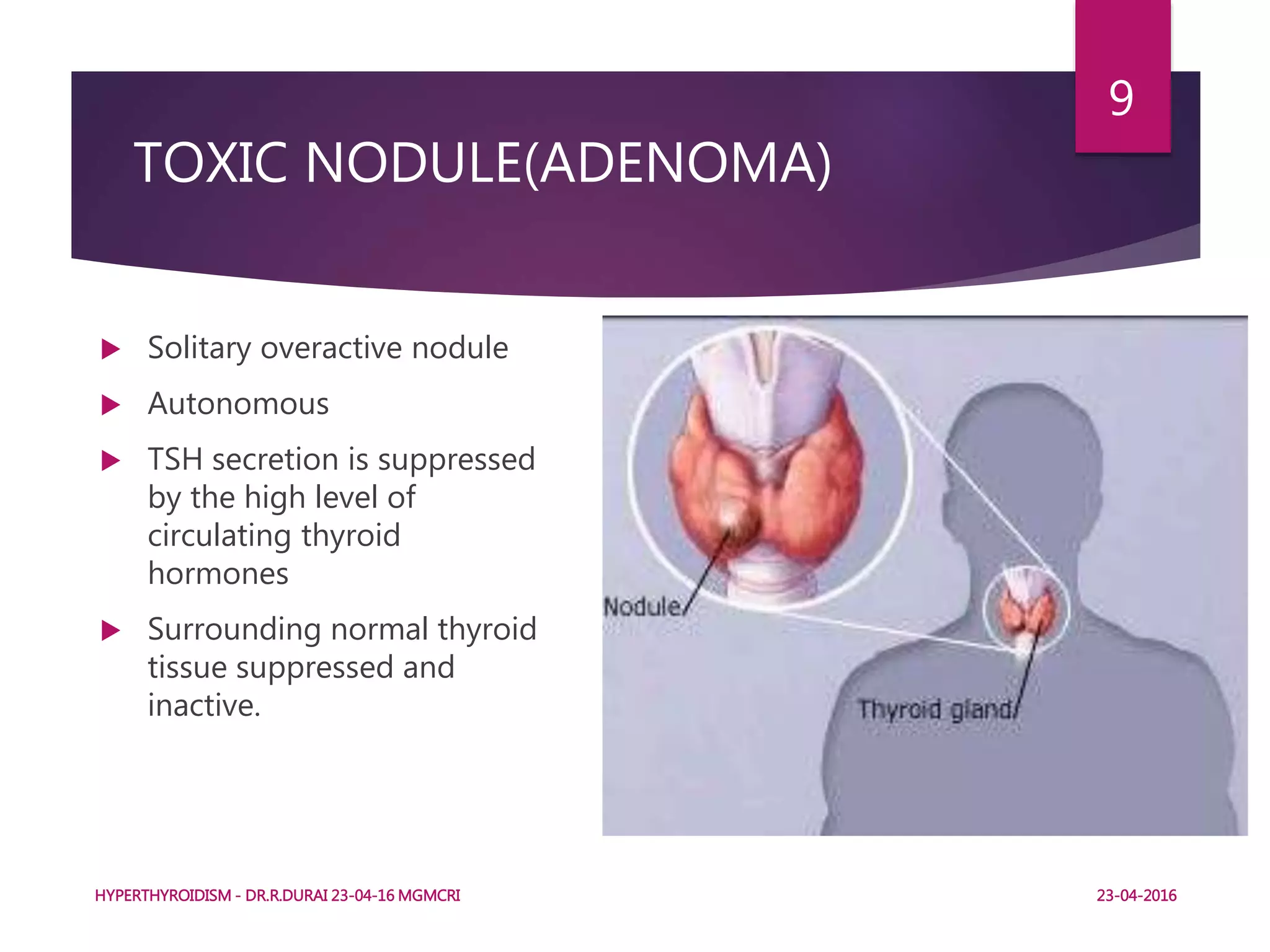
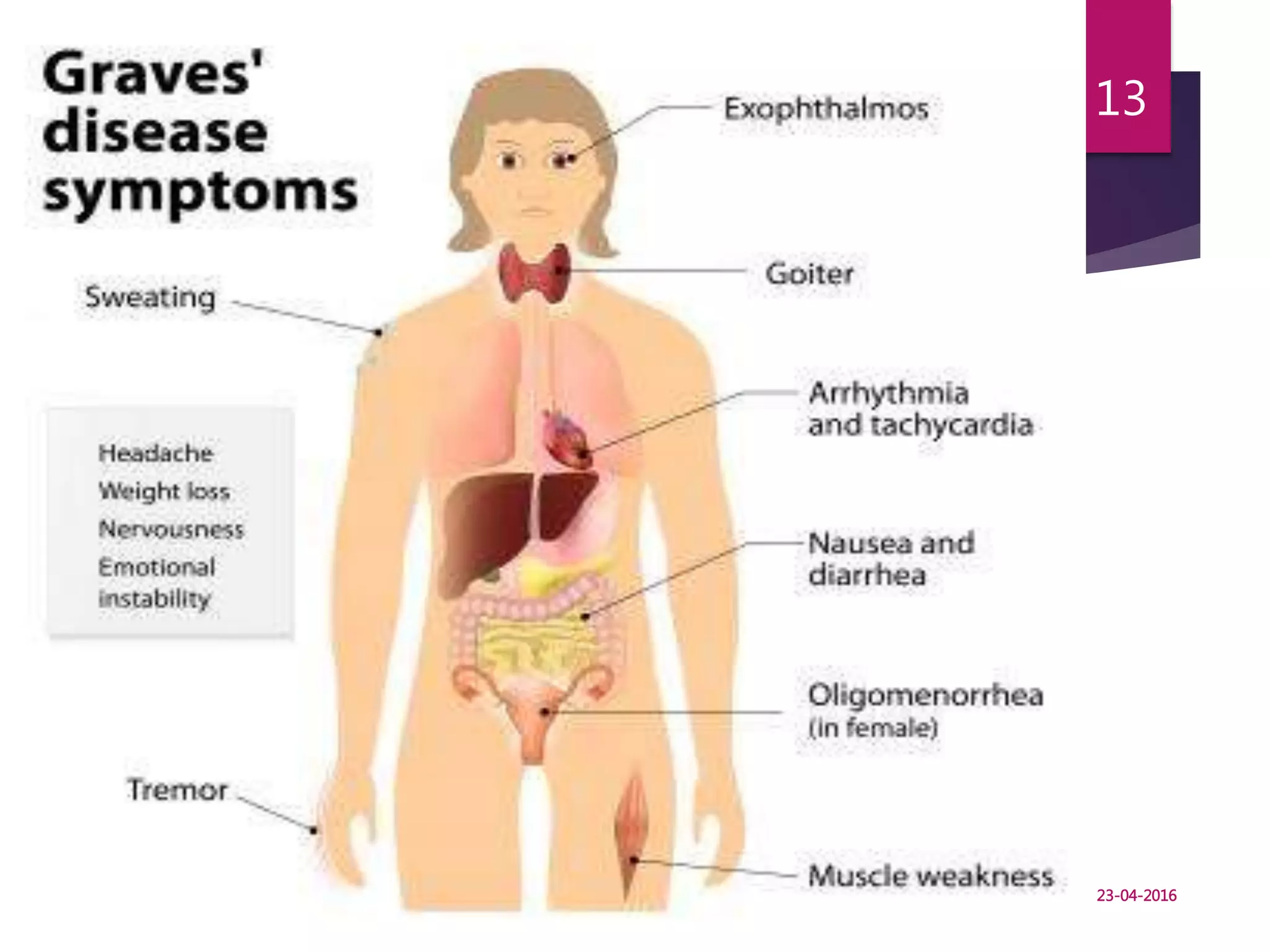
This document discusses hyperthyroidism and its treatment. It defines hyperthyroidism as increased secretion of thyroid hormones due to various stimuli. It then describes the clinical types of hyperthyroidism including diffuse toxic goitre (Graves' disease), toxic nodular goitre, and toxic nodule. The document outlines the symptoms, diagnosis, and principles of treatment for hyperthyroidism including anti-thyroid drugs, radioactive iodine therapy, and surgery. Treatment options depend on factors like the type and severity of hyperthyroidism, patient age and preferences.