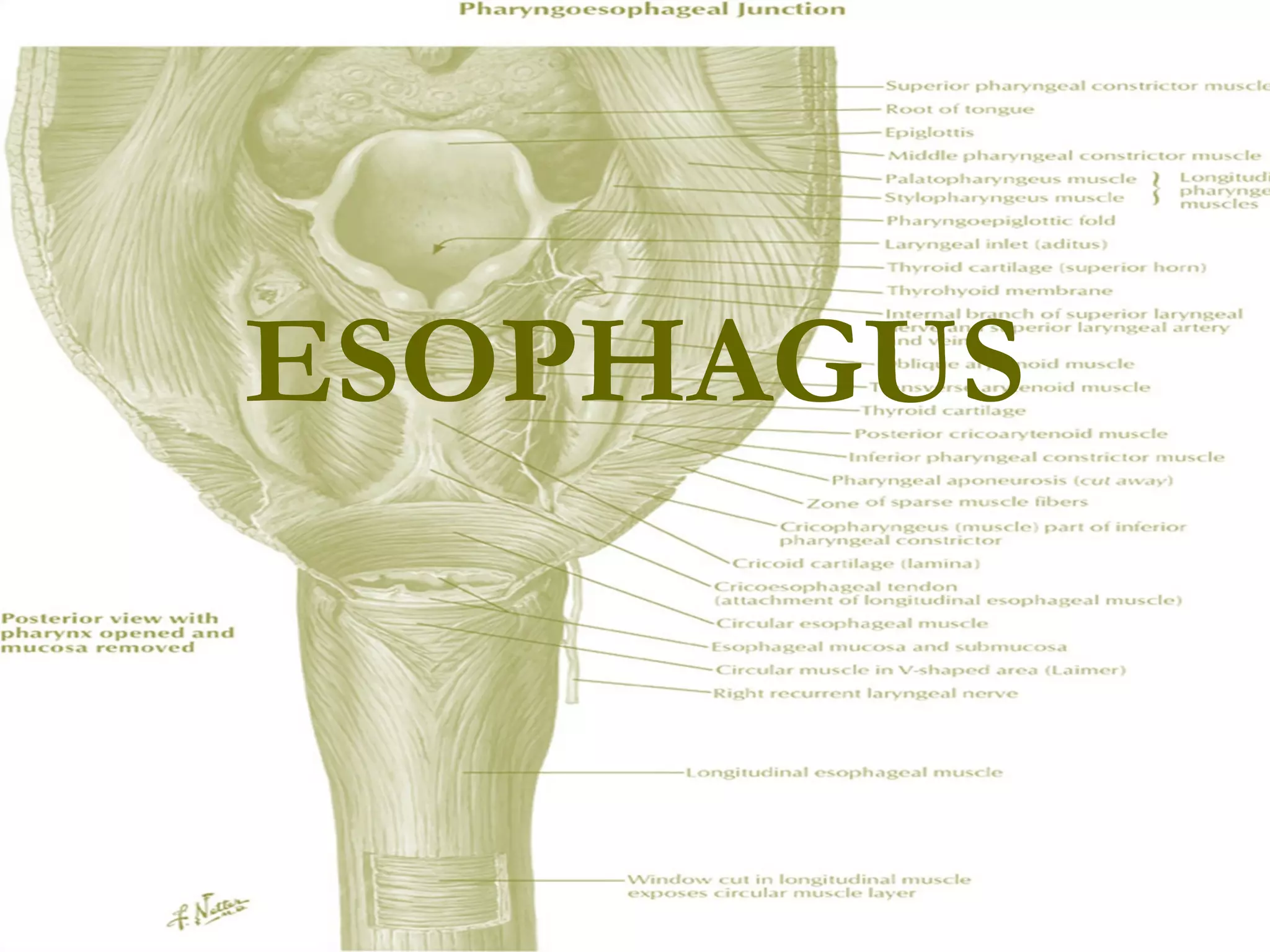
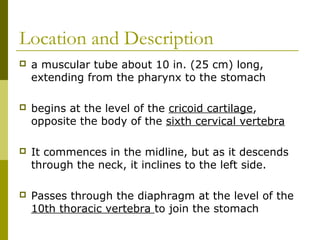
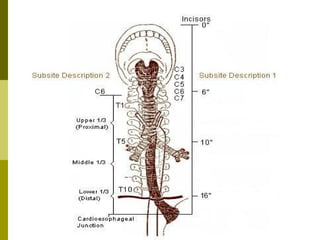
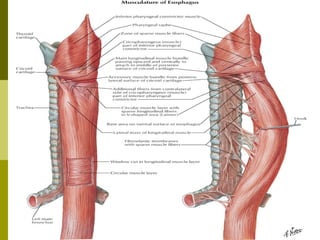
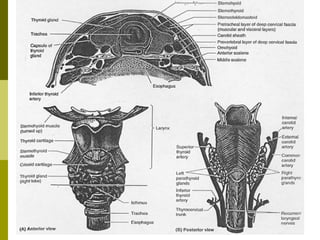
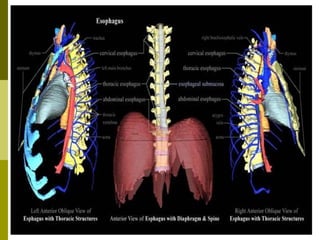
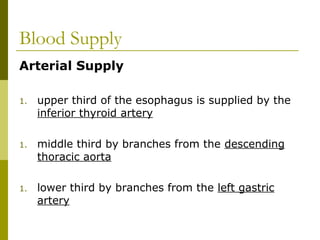
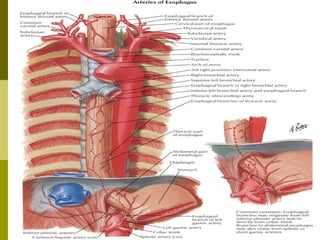
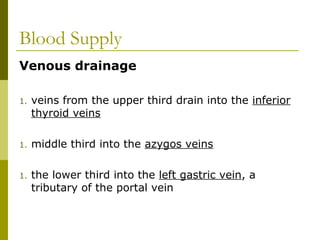
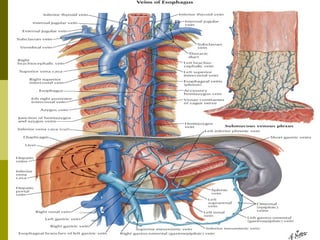
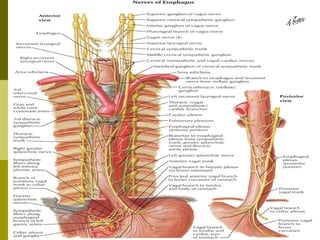
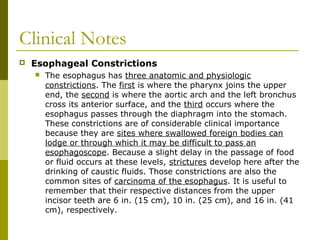
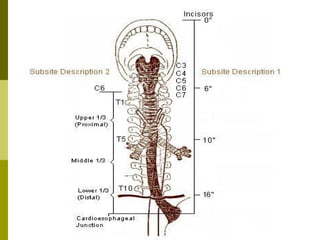
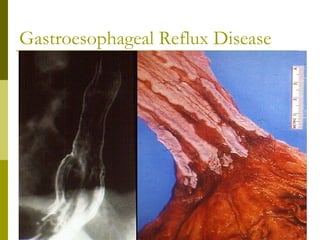
The esophagus is a 10 inch muscular tube that extends from the pharynx to the stomach. It begins at the level of the cricoid cartilage and passes through the diaphragm to join the stomach. The esophagus has circular and longitudinal muscles and receives its blood supply from branches of the inferior thyroid, descending thoracic aorta, and left gastric arteries. It drains into the inferior thyroid, azygos, and left gastric veins. The esophagus has three anatomical constriction points that are common sites for food impactions and carcinoma. Gastroesophageal reflux disease is the most common esophageal disease and causes irritation from stomach acid in the esophagus.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


